Compatibility: Libra woman and Leo man
Representatives of these zodiac signs do not always become close people, but they are pleasant and interesting to each other. Unites...
POSTHEATED CHANGES (cadaveric changes, cadaveric phenomena) - a set of changes that develop after death as a result of the cessation of the vital functions of the body.
P. and. appear at different times, so they are conventionally divided into early (cooling of the corpse, cadaveric spots, rigor mortis, drying out, autolysis) and late (transformative, or transformative), as a result of which the corpse is subjected to decomposition and destruction (autolysis, rotting) or natural preservation (mummification, saponification, peat tanning, freezing). P.'s development and. depends on the nature of clothing, environmental conditions, the degree of blood loss, the development of subcutaneous tissue, the cause of death, possible concomitant diseases and conditions of the body, and a number of other exogenous and endogenous factors.
Patterns of appearance and development, taking into account the dynamics of P. and. used in forensic medicine to diagnose the fact of death (see) and determine the period of limitation of its occurrence, establish the initial position of the corpse and its possible change in the postmortem period, for an approximate judgment about the cause of death and the resolution of certain other special issues. P. and. are also essential for studying the survival time of certain organs and tissues when determining their suitability for transplantation (see Transplantation). Knowledge of the characteristics of the decomposition of a corpse is necessary for differential diagnosis of putrefactive changes with intravital injuries or diseases. Thus, the protrusion of the tongue from the oral cavity under the pressure of accumulated gases imitates one of the signs of mechanical asphyxia; the formation of blisters on the skin of a corpse due to detachment of the epidermis and accumulation of fluid resembles a second degree burn; the greenish-colored putrefactive venous network is similar to the so-called. lightning figure; the flow of gastric contents into the respiratory tract imitates intravital aspiration of vomit; the release of bloody fluid formed during decay is similar to uterine, gastric or pulmonary bleeding. Putrefactive imbibition and hardening of the lungs should be differentiated from pneumonia, and changes in the gastric mucosa, its apparent swelling and red-brown color, should be differentiated from changes found in poisoning. Poisoning with caustic poisons can simulate rupture of the stomach wall under the influence of putrefactive gases. Putrefactive imbibition, compaction and red-brown color of the pancreas may resemble morphol, a picture of hemorrhagic pancreatitis. Foamy blood due to the penetration of putrefactive gases into the vessels is similar to blood during an air embolism (see). The deposition of crystals of hydroxyphenylammonium propionic acid salts on the fascia and serous membranes of internal organs should be distinguished from the deposition of crystals of poison taken during life.
Knowledge of the patterns of development of P. and. has significant atheistic significance, helping to expose superstitions associated with dying and death, burial of the so-called. supposedly dead. The movement and change in the position of the corpse in the coffin is explained by the non-simultaneity of the process of decay in different parts of the body, the varying degrees of severity of cadaveric emphysema in them. Posthumous birth, usually accompanied by uterine inversion, is caused by an increase in pressure inside the abdominal cavity due to the formation of putrefactive gases. Knowledge of the patterns of fat wax formation and mummification of corpses makes it possible to exclude the divine origin of holy relics used by clergy as an object of worship for believers.
Cooling the corpse. After the cessation of cardiac activity, body temperature usually remains at the same level for the first tens of minutes, then begins to gradually decrease - on average by 1° per 1 hour at an ambient temperature of 16-18°. Over time, due to the evaporation of moisture from the surface of the skin, the temperature of the corpse reaches values 0.5-3° below the ambient air temperature; if it is less than -4°, cooling turns into freezing. The speed and degree of cooling are influenced by the ambient temperature, humidity and wind strength when the corpse is in the air, the nature of the environment, the posture of the corpse, the degree of fatness, and the cause of death. In case of death from tetanus, sepsis, typhus, or certain poisonings, the body temperature after cardiac arrest may rise for a short time to 40-41° or more. Cooling of newborn corpses occurs very quickly due to the tenderness and thinness of the epidermis, the larger surface of the skin in relation to the weight (mass) of the body. Registration of cooling of the corpse in forensic medicine. In practice, it is carried out by repeated rectal thermometry or deep electrothermometry of the liver. Body temperature less than 20° is a reliable sign of death. Taking into account the dynamics of cooling of the corpse in each specific case, the duration of the post-mortem period can be established.
Cadaveric spots- a peculiar coloring of the skin due to the flow and accumulation of blood in the underlying areas of the body. They begin to form 2-4 hours after the cessation of cardiac activity. The degree of their severity depends on the rate of death of the organism; Thus, abundant diffuse saturated cadaveric spots are characteristic of rapid death (mechanical asphyxia, acute coronary insufficiency); scanty pale - for death from heavy blood loss, with prolonged agony, severe exhaustion of the body. Typically, cadaveric spots are blue-violet or purple-violet in color. Their scarlet, red color indicates poisoning with carbon monoxide, hydrogen sulfide, cyanide, death from hypothermia; grayish-brown - for poisoning with methemoglobin-forming poisons (Bertholometa salt, nitrites). It is customary to distinguish 3 stages of development of cadaveric spots: hypostasis (from their appearance until 12-14 hours after death), diffusion, or stasis (from 12-14 hours until the end of the first day), and imbibition (more than one day). Hypostasis is characterized by overflow of the veins with blood, stasis by hemolysis of red blood cells and diffusion of the liquid part of the blood through the wall of blood vessels, the beginning of staining of surrounding tissues with blood pigment; imbibition - the completion of tissue staining with blood. When you press a finger (dynamometer) on the cadaveric spot in the stage of hypostasis (see), it completely disappears and is restored again after the load is removed in a few seconds. When the corpse is turned over, the cadaveric spots at this stage completely disappear and reappear in the underlying areas of the body. In the stasis stage, cadaveric spots turn pale when pressed, but do not disappear completely; the original color is restored slowly (within several minutes). When a corpse is turned over, cadaveric spots remain both in the same places and are formed on new, underlying areas of the body (color book Fig. 4). In the stage of imbibition (see), cadaveric spots do not change color when pressed; when the corpse is turned over, they are preserved only in the places of their initial formation. Simultaneously with the appearance of cadaveric spots on the skin, the formation of the so-called. cadaveric hypostases in the underlying parts of the internal organs, which gives them a reddish-bluish tint due to accumulated blood. The presence of cadaveric spots is a reliable sign of cardiac arrest, and their nature allows us to judge how long ago death occurred, indicates a change in the initial position of the corpse, and provides guidance in the diagnosis of certain causes of death.
Rigor (muscular) mortis- a kind of compaction and shortening of skeletal muscles, creating an obstacle to passive movement in the joints, as well as the smooth muscles of internal organs and the muscles of the heart. Rigor mortis begins to manifest itself externally 2-4 hours after the heartbeat stops, reaches its maximum severity by the end of the 1st day of the post-mortem period and spontaneously resolves on the 3rd-4th day. It is based on a violation of ATP resynthesis and the accumulation of lactic acid. Complete breakdown of ATP in the muscles occurs only after 10-12 hours. after cardiac arrest, therefore rigor mortis, which was artificially disturbed before this time, is completely restored, which must be taken into account in forensic medicine. practice (the possibility of simulating lifetime actions for criminal purposes). Rigor mortis develops faster at a higher (but not higher than 50°) ambient temperature and low humidity, in persons with well-developed muscles, with vigorous muscular work preceding death, convulsions, poisoning with substances acting on the c. n. With. (strychnine, pilocarpine, etc.). Sepsis, severe debilitating diseases preceding death, some poisonings (chloral hydrate, toadstool) cause weak expression or complete absence of rigor mortis. In rare cases (destruction of the substance of the medulla oblongata, sharp convulsions preceding death), the so-called. cataleptic rigor mortis, which develops at the moment of cardiac arrest as a result of the direct transition of intravital contractures into rigor mortis and, thus, preserving the person’s posture at this moment. In forensic medicine, rigor mortis is determined by the presence of resistance to passive movements in the joints of the limbs, neck muscles and masticatory muscles. Rigor mortis is a reliable sign of death; it allows one to judge how long ago it occurred, the initial position, and in some cases the cause of death.
Drying due to uncompensated evaporation of moisture from the surface of the skin, it begins immediately after death, but visually it appears only after a few hours. The process begins in areas devoid of epidermis, i.e. on the mucous membranes of the eyes, lips, genitals, or in those places where the epidermis is thinnest - the scrotum, the terminal phalanges of the fingers. The first sign of drying out and, therefore, a reliable sign of death is the formation of dull yellowish-gray or brownish areas of drying of the sclera of the eyes in the form of isosceles triangles, the base facing the iris, the apex towards the corners of the eyes - Larcher spots. They appear especially clearly if the eyes remained open after death. Subsequently, the areas become denser, wrinkle, acquire a brownish, purple color and other drying areas. Drying also develops rapidly in those areas where the epidermis was damaged shortly after death; “parchment” spots form in these places - dense brownish-yellow sunken areas of the skin with translucent red vessels. The formation of parchment spots is also possible on intact skin in places that have been subjected to prolonged pressure. The drying process (see Mummification) is accelerated under conditions of high temperature and low humidity of the surrounding air. Usually it is limited to certain areas of the body, but under special environmental conditions, drying out can be total, which leads to mummification of the corpse (color fig. 7 and 8).
Autolysis- disintegration of body structures under the influence of hydrolytic enzymes due to the disorganization of enzyme systems occurring after death and a shift in pH to the acidic side. Externally, this process is characterized by a gradual softening and liquefaction of organs and tissues, the severity of which depends on the quantitative content of proteolytic enzymes in them. The high content of lysosomal enzymes in the pancreas, adrenal glands, spleen, and liver causes the appearance of initial signs of autolysis in these organs. Blood undergoes fairly rapid autolysis - post-mortem hemolysis is essentially a manifestation of autolysis. In the stomach and small intestine, digestive juices containing pepsin, trypsin and other enzymes are of leading importance. After death, their action is directed to their own mucous membrane, which has lost its protective barrier functions. Thus, self-digestion (see) of the mucous membrane occurs, the intensity of which is directly dependent on the stage of digestion that took place immediately before death. Self-digestion is most often limited to the mucous membrane, but in infants the walls of the stomach and intestines may be involved in the process of autolysis. Under certain conditions, gastric juice can enter the esophagus, pharynx, even trachea and cause esophagomalacia, “acid” softening of the lungs.
Rotting - a complex biol, a process caused by numerous microorganisms that intensively multiply in the corpse and secrete a large number of proteolytic enzymes that decompose organic substances, primarily proteins, fats and carbohydrates. Putrefactive decomposition (transformation) of a corpse can occur in two forms. The first is observed when rotting occurs according to the type of reduction reactions, accompanied by the formation of simple volatile hydrogen compounds, which, as a rule, have an unpleasant odor. This process is considered to be rotting itself (see). The second form occurs when decomposition occurs by oxidation or combustion with the formation of a number of acid-containing compounds. This process is called smoldering. Typically, the putrefactive decomposition of a corpse consists of 3 stages: the formation of gases, softening of tissues followed by their imbibition and their complete liquefaction. Both aerobic and anaerobic saprophytes take part in the decay process; pathogenic microbes usually die quickly. Therefore, it is believed that infection inf. diseases during the autopsy of a corpse in the stage of decay is impossible. At the same time, during the process of decay, some toxic substances of the ptomaine group (putrescine, cadaverine) are formed, called cadaveric poison, which requires some caution when examining putrefactively altered corpses. The speed and characteristics of decay depend on a number of external and internal factors. High (approx. 40°) ambient temperature and high humidity contribute to the development of the rotting process. Rotting develops quickly in air, more slowly in water, and even more slowly in soil. At temperatures below 0° and above 50-60°, with a sufficient supply of dry air, rotting can slow down sharply and stop altogether. The process of decay is significantly accelerated during death from sepsis, purulent diseases or inf. diseases. Gender, age, and level of nutrition also matter. The corpses of newborns decompose faster, the corpses of old people - more slowly. The corpses of men decompose faster than the corpses of women, of obese people faster than of thin ones. In case of death from asphyxia, sun and heat stroke, or electrical injury, the process of decay develops quickly, in case of death from debilitating diseases associated with dehydration, in case of poisoning with alcohol, arsenic, quinine, cyanide, sublimate, etc., it develops slowly. The development of putrefaction is significantly delayed if a person consumes a large amount of antibiotics (tetracycline) and sulfonamide drugs shortly before death. In just 3-6 hours. after death, putrefaction begins to develop in the large intestine, where a large amount of putrefactive gases are formed, a number of which (hydrogen sulfide, methyl and ethyl mercaptan) have a specific unpleasant odor. Hydrogen sulfide, combining with hemoglobin in the blood, forms sulfohemoglobin and iron sulfide, which have a dirty green-brown color. Initially (days 1-2), a greenish color appears in the iliac regions, then along the course of large vessels, forming a putrefactive venous network (color. Fig. 6). On the 5-7th day, putrefactive gases, penetrating into the subcutaneous tissue, seem to swell it, leading to the development of cadaveric (putrefactive) emphysema, especially in the area of the face, lips, mammary glands, abdomen, scrotum, and limbs. When touching the skin of such a corpse, a sharp crepitus is felt. On the 10-12th day, the entire skin takes on a dirty green color. Subsequently, the epidermis begins to peel off with the formation of blisters with serous-bloody contents, after rupture of which a moist brownish-red surface is exposed (tsvetn. Fig. 5). Of the internal organs, the stomach, intestines, lungs, liver, brain, pancreas, kidneys, adrenal glands, and heart are the most susceptible to rotting. The organs become as if “foamy”, acquire a brownish-red, and then a brownish-green or dirty green color (putrefactive imbibition), and liquefy. When gistol, examination in the tissue of these organs fails to identify parenchymal elements. Gradually, the process of decay spreads to other organs and tissues, with the non-pregnant uterus, prostate gland, ligaments, and cartilage surviving the longest.
Depending on the burial conditions (the nature of the soil, its pollution, humidity), after approximately 2 years the tissues and organs take on the appearance of a disintegrating homogeneous dirty-gray mass, the edges gradually dissolve and are washed away by soil water. Skeletal bones can be preserved indefinitely. Putrefactively altered corpses can be the object of forensic medicine. examination, while the degree of putrefactive decomposition is not an obstacle to forensic medicine. examination of the corpse (see Exhumation). Even with pronounced decomposition of the corpse, various damage can be detected, especially to bones, gunshot marks on the skin, etc., which is of important expert diagnostic value.
Preservative forms can determine the preservation of appearance (freezing) or individual characteristics, allowing for personal identification (see), identifying the characteristics of previously received injuries, etc. These types of P. and. include complete drying of the corpse or its parts (natural mummification), saponification of the corpse, or saponification (see Fatwax), peat tanning, etc. (color fig. 9).
Peat tanning occurs when a corpse gets into peat bogs and soils containing humus and other acidic, tannic and astringent substances. At the same time, the skin of the corpse thickens, acquires a dark brown color, and the internal organs decrease in size. Under the influence of humus compounds, mineral salts dissolve and are washed out of the corpse, so the bones acquire the consistency of cartilage and are easily cut with a knife. With histol. The study reveals complete preservation of the structure of the skin, muscles, and nervous tissue. In peat bogs, corpses persist indefinitely. At their court.-med. The study makes it possible to determine damage received during life. Corpses can also be preserved for a long time in water with a high salt content or in oil.
To P. and. The destruction of a corpse also includes its destruction by representatives of the plant (mold) and animal (insects, rodents, small and large predators, etc.) world. Molds and molds can grow on corpses or parts thereof if there is sufficient moisture. The participation of molds in the destruction of a corpse is insignificant, but some of their species can provide valuable indications about the place where the corpse was located and how long ago the death occurred. Of the insects, flies are the most important. Soon after death, they begin to lay large numbers of eggs in the form of white grains around natural openings, eyes, and wounds. After 1 day, larvae form from them, secreting a fast-acting proteolytic enzyme that melts the soft tissues of the corpse. Penetrating inside the corpse, they continue their development for 1.5-2 weeks, after which pupae are formed, and after another 2 weeks - flies. Thus, biol, the development cycle of flies is 3-4 weeks, but at elevated temperatures it can accelerate to 2 weeks. (at an ambient temperature of 30°), at low temperatures it lengthens significantly. Under favorable conditions (air temperature 15-20°), flies can completely destroy the soft tissues of the corpse of a newborn in 1.5-2 weeks, and an adult in 1-1.5 months. Other insects can also damage a corpse, in particular ants (they can skeletonize the corpse of an adult within 2 months), beetles, and mites. It is believed that the soft tissues and fat of corpses that are in the ground for 1-3 months are eaten by sarcophagi, by skin beetles for 2-4 months, and by sylphs for 8 months. Cartilage and ligaments are destroyed by mites.
Quite often, corpses are destroyed by rodents, especially rats, as well as wolves, jackals, and less often cats and dogs. Damage in these cases usually has an irregular shape with torn, scalloped, bloodless edges, on which tooth marks are clearly visible. In the aquatic environment, corpses are damaged by some types of predatory fish, crayfish, and leeches. Some birds, for example, crows, also destroy corpses. Damage to corpses by animals complicates the examination, but is not an obstacle for forensic medicine. corpse research.
Bibliography: Avdeev M.I. Forensic medical examination of a corpse, M., 1976; Lushnikov E. F. and Shapiro N. A. Autolysis, Morphology and mechanisms of development, M., 1974; Melnikov Yu. L. and Zharov V. V. Forensic medical determination of the time of death, M., 1978; Multi-volume manual on pathological anatomy, ed. A. I. Strukova, vol. 1, p. 636, M., 1963; Strukov A. I. and Serov V. V. Pathological anatomy, M., 1979; Forensic Medicine, ed. V. M. Smolyaninova, M., 1980.
I. V. Buromsky, M. N. Lanzman.
Students, graduate students, young scientists who use the knowledge base in their studies and work will be very grateful to you.
Introduction
Chapter 1. The Dying Process
Conclusion
Introduction
Forensic medicine is a branch of medicine that resolves medical and biological issues that arise during the activities of forensic investigative bodies, and also assists health authorities in improving the quality of their work. Forensic medicine is not a random, mechanical collection of medical disciplines used for targeted legal practice, as it was at the beginning of the development of forensic medicine.
Currently, forensic medicine is an independent medical science that studies a certain range of issues and has its own research methods. As forensic medicine developed, a number of sciences emerged from it as independent disciplines, for example, forensic chemistry, forensic psychiatry, and forensic toxicology. Forensic medicine is connected with all other medical sciences, these are pathological physiology, pharmacology, surgery, histology, traumatology. How medical science uses laboratory research methods, X-ray, microbiological, and physiotechnical research methods. With the help of the latter, for example, the type of weapon, the mechanism of injury, and the establishment of the intravital origin of the injury are determined.
Among the legal sciences, criminology is very close to forensic medicine, which is a legal discipline that studies the tactics, methods and techniques of crime investigation. In order to successfully conduct an investigation or trial, and correctly evaluate an expert’s opinion, a lawyer must have an understanding of the capabilities of forensic medicine and the limits of the competence of forensic medical examination. Under this condition, he will be able to correctly select the right experts, formulate questions for the experts, and critically evaluate their conclusions. Often, the investigator himself has to examine the corpse at the scene of the incident, and having knowledge of the basics of forensic medicine, the investigator will be able to navigate in determining how long ago the death occurred, the nature of the injuries, and the features of the incident.
The system of the subject is determined by the existing practice of forensic medical examination and can be presented in the following form: the parocessual part, which sets out the rules for conducting a forensic medical examination, provides the content and interpretation of various laws, regulations, instructions relating to forensic medical examination; the material part, which sets out medical and natural scientific information that makes up the content of forensic medicine as a science. This part is divided into several sections:
1. Department of the doctrine of death (Thanatology) - includes the doctrine of death, its occurrence, its signs, post-mortem changes on the corpse, the difference between violent death and death causing suspicion of violence. This also includes techniques for forensic medical examination of corpses.
2. Department of injuries (forensic traumatology): - includes the study of various injuries, their recognition and precise characteristics, determination of their effect on the body, clarification of the methods and circumstances of injury and their legal assessment.
3. Department of poisoning (forensic toxicology) - poisonings that are important in forensic medicine are studied, as well as their clinical recognition, treatment and prevention.
4. Department of controversial sexual conditions - includes questions regarding sexual functions, determination of infection with sexually transmitted diseases, all types of research regarding violations of sexual integrity (rape, molestation), determination of the child's identity.
5. Pregnancy and childbirth (forensic obstetrics) - studies ways to recognize pregnancy, its duration, recognition of births that have taken place, methods of abortion. This section also includes a chapter on infanticide.
6. Department of forensic medical examination of material evidence - studies biological evidence: blood, semen, hair and interpretation of its results.
7. Border areas of criminology and forensic medicine - forensic technical examination - these are methods of personal identification, feigned and artificial diseases, and determination of the type of death.
8. Department for the study of medical practice and other types of medical work, medical errors and medical practice.
9. The department for the study of mental state (forensic psychiatry) is developed by psychiatrists, studying methods for determining sanity, various mental illnesses that exclude or mitigate criminal liability or interfere with a person’s civil capacity.
There are two main tasks of forensic medicine:
1. Assistance to the justice authorities.
2. Providing medical and preventive care to the population. In accordance with the order of the USSR Minister of Health N166 dated April 10, 1962, it requires forensic medical examiners to: discuss forensic cases at clinical and anatomical conferences, notify health authorities about facts of gross discrepancies in clinical and anatomical diagnoses and defects in medical work; carrying out analyzes of cases of sudden death, transport injuries, domestic and industrial poisoning, in order to carry out preventive measures and identify defects in medical care.
Chapter 1. The Dying Process
The science that studies the issues of death and dying is called thanatology (from the Greek death - thanos). The dying process can be quick or it can be long. There are several periods in the dying process.
1. Preagonal state: weak, rapid pulse, pale or spotted skin, shallow, rapid breathing. During this period, the body tries to turn on compensatory mechanisms aimed at maintaining and normalizing basic life functions. The preagonal state can last for several hours, even if no medical treatment is provided.
2. Agonal state: the beginning of agony (not in all types of dying) is very clearly registered by a terminal pause. It is characterized by the fact that after rapid breathing, it suddenly stops completely. The pause lasts up to 2 - 4 minutes. Following this, agony begins directly, including a single shallow breath, the amplitude of respiratory movements increases, the person seems to gasp for air. Due to a violation of the respiratory act, breathing stops completely. The cerebral cortex turns off, although at the supomolecular level the processes of life are mobilized and continue. The appearance of the dying person changes sharply: the face becomes pale, sallow, the nose is pointed, the cornea loses its luster, and the mouth opens slightly.
3. Clinical death: begins from the moment the activity of the cerebral cortex, breathing, and blood circulation ceases and lasts 4 - 7 minutes, during which resuscitation measures are most often carried out. Determining the fact of death is the most important moment in the work of a forensic doctor, and even more important in the work of the attending physician. It is not difficult to determine the fact of death 6 - 8 hours after its occurrence, when obvious cadaveric phenomena appear. It is difficult to navigate the first 1 - 2 hours. In a hospital setting, this issue is not difficult to resolve since there is a variety of equipment, however, in accordance with the existing situation, the corpses of persons who died in the hospital are transferred to the morgue no earlier than 2 hours after death, that is, no earlier than absolute signs of death appear on the corpse - cadaveric spots. Currently, to ascertain death, indicative and reliable signs of death are used. Orienting factors include: motionless body position, pale skin, lack of consciousness, breathing, pulse, heartbeat, lack of sensitivity to painful stimuli, lack of pupillary reaction to light. When working at the scene of an incident, a forensic expert most often does not have doubts about the fact of death, since by this time the absolute signs of death are clearly visible: the presence of cadaveric spots and rigor mortis, a decrease in body temperature below + 20 degrees, drying of the sclera and cornea, a sign Beloglazova (change in the shape of the pupil when pressed - cat's eye).
Chapter 2. Early cadaveric changes
Cadaveric phenomena are divided into early (on the 1st day after death) and late (become noticeable from the 2nd day). The early ones include:
1. Cooling.
2. Drying.
3. Cadaveric spots.
4. Rigor mortis.
5. Autolysis.
1. Cooling of the corpse - for diagnosing the duration of death, it has only approximate knowledge, since, along with other factors, it is not yet known what the body temperature was at the moment of dying, and it can fluctuate within significant limits not only in patients, but also in healthy people .
Heat production in the body of the deceased stops and the corpse cools down to ambient temperature. The temperature of the corpse may be lower than the ambient temperature due to the evaporation of moisture. The process is usually completed by the end of the first day. Exposed areas (hands, face) cool faster, their cooling can be noticed after 1 - 2 hours, the armpit is slower. It is recommended to measure temperature in the rectum and deep thermometry (liver) using an electric thermometer with special needle sensors.
Heat transfer depends on external conditions: air temperature, humidity, ventilation, clothing and its nature. Individual characteristics also matter: the development of subcutaneous fat (possessing low thermal conductivity, it slows down cooling), age (faster in children), cause of death (faster in case of alcohol or arsenic poisoning, blood loss accelerates), so the results of thermometry have very relative values .
After death occurs, the process of establishing a thermal balance between the temperature of the dead body and the ambient temperature occurs. For example, if the ambient temperature is higher than the temperature of the dead body, then the corpse heats up; if it is lower, the corpse cools down. The greater the temperature difference between the corpse and the environment, the more intense the cooling (or heating) process. The process of changing the body temperature of a corpse is influenced by the following factors: age, physique, position (posture) of the body, the nature and amount of clothing, cause of death, air movement, humidity and other factors. It is generally accepted that at an ambient temperature of 18 °C, a corpse cools down by 1 °C per hour, and by the end of the day it reaches ambient temperature.
At the present stage, the study of the process of cooling a corpse is the most objective way to establish the duration of death.
Devices based on the ETM-ZB electric thermometer make it possible to measure the temperature in the body of a corpse with an accuracy of hundredths of a degree. It is necessary not only to accurately measure the temperature in the body of a corpse, but also to establish the dynamics of its change within 1-3 hours. The best results are obtained by so-called deep thermometry, for example, inserting a flexible temperature sensor into the esophagus to the level of the diaphragm, as well as studying the temperature in the liver tissue. Measuring the temperature in the rectum gives satisfactory results. For more complete reliability, it is necessary to carry out measurements repeatedly at time intervals.
2. Corpse desiccation. The process of drying of the skin (exposed areas of the body) and mucous membranes (cornea of the eyes, mucous membrane of the mouth, mucous membrane of the labia minora) is observed immediately after death and depends, first of all, on environmental conditions. The intensity of the drying process increases sharply under conditions of elevated temperature. When the eyes are open, the cornea in the shape of a triangle (Larche's spots) dries out and becomes cloudy; the border of the lips of the mouth is dense to the touch and dark red in color. The mucous membrane of the protruding tip of the tongue becomes dense to the touch and red-brown in color during mechanical asphyxia. The skin of the scrotum (or the mucous membrane of the labia minora) may also dry out in the absence of underwear; it becomes dense to the touch and red-brown in color. In areas of the skin, especially in thin places (hands) that have been subjected to compression, areas of drying out can be found, which give the impression of intravital abrasions or bruises. To establish the survival of these formations, it is necessary to place a gauze napkin soaked in water for 2 - 3 hours. After soaking in water, such an area of parchment density turns pale and disappears, while intravital damage remains almost unchanged.
Drying flutters due to the evaporation of moisture from the surface of the body. Evaporation of moisture is a physiological, constantly compensated process that occurs in a living organism. After death, the physiological balance between loss and replenishment of fluid is disrupted, and the body begins to lose moisture through condensation and evaporation.
In places that are most moist during life (lips, sclera), drying is intense and is presented in the form of areas of parchment density. The speed and intensity are influenced by environmental conditions - air temperature, air movement and individual characteristics - degree of nutrition, dehydration, clothing.
Drying of the skin and mucous membranes begins immediately after death, but visually manifests itself after a few hours. It begins with the corneas of open or slightly open eyes (Larchet's spots - drying out in the shape of a triangle 4 - 5 hours after death). The epidermis protects the skin from drying out, so where it is damaged, conditions for drying are created (abrasions, furrows). The lack of a direct relationship between the rate of drying and the period after death, as well as many influencing factors, prevent its use for diagnosing the duration of death.
3. Cadaveric spots - after the cessation of cardiac activity, blood flows under the influence of gravity to the lower parts of the body. Vessels that have lost their tone dilate and fill with blood. Corpse spots appear after 2 - 3 hours.
After death, blood and lymph move under the influence of gravity to the lower parts of the body and organs. The blood vessels in these sections passively expand under fluid pressure. And after 1 - 2 hours, the blood-filled vessels of the skin and subcutaneous fat give the skin first a light purple color, and then a dark purple color, that is, a cadaveric spot is formed. The skin of the body in the overlying parts of the corpse becomes pale due to the movement of blood.
In the formation of cadaveric spots, 3 stages can be distinguished: hypostasis, stasis and imbibition.
1. Hypostasis. Cadaveric spots form immediately after cardiac arrest, the most intensive development occurs in the first hours (2 - 4 hours). When the position of the corpse changes during these hours, blood moves from the places of primary formation of cadaveric spots and the appearance of new ones on other, lower lying parts of the body. In areas of the body of a corpse that are pressed to the plane (interscapular, lumbar and gluteal regions, the back of the thigh and lower leg), cadaveric spots do not form due to compression of the blood vessels containing blood. Due to this mechanism, the pattern of clothing folds is also clearly visible against the background of the formed cadaveric spots. The color and severity of cadaveric spots are influenced by the following factors: cause of death, type of death, duration of dying, condition and amount of blood in the body, and others. As a rule, cadaveric spots have a dark purple color, but when poisoned by various compounds, their color may change. In case of poisoning with carbon monoxide or hydrocyanic acid compounds, the blood becomes bright red and due to this, the cadaveric spots have a red-pink color. When poisoned by poisons (aniline dyes, nitrobenzene and others), cadaveric spots become grayish-brown, and when poisoned by hemolytic poisons (arsenic compounds, many types of fungi, and others), cadaveric spots have a jaundiced tint. When the body contains a small amount of blood, as a rule, with heavy blood loss or when the blood in the vessels is in a state of coagulation, cadaveric spots turn out to be weakly expressed and are presented in the form of local or merging areas.
2. Stasis. Blood hemolysis products gradually diffuse through the vascular wall into the surrounding tissue. Compression of blood vessels over time causes the effect of blanching of the cadaveric spot to a lesser extent. The movement of the body of a corpse and its turning over 6 - 18 hours after death reveals an important forensic circumstance: the cadaveric spots that formed initially and ended up in the overlying sections during the turning over do not completely disappear, and the degree of their blanching decreases over time. New cadaveric spots appear on the underlying areas of the corpse. Their intensity is less, the later the corpse was turned over. After 12 - 15 hours, the plasma sweats, hemolysis products permeate the tissues, the blood thickens, so the cadaveric spots turn pale when pressed and partially move.
3. Imbibition. After the first day, when the corpse is turned over, the cadaveric spots where they formed previously do not disappear and do not form in new places. This principle is the basis for one of the methods for establishing the age of formation of cadaveric spots and, thereby, determining the age of death. To do this, a specially designed dynamometer is used to apply pressure with a force of 2 kilograms per 1 square centimeter with an exposure of 3 s to the area of the cadaveric spot, and then determine the time for restoration of the color of the blanched area to the level of color intensity of the surrounding skin. After 24 - 35 hours, red blood cells disintegrate and the surrounding tissues become saturated with plasma containing hemoglobin. They do not fade or disappear. Cadaveric spots depend on the condition of the blood: liquid blood - cadaveric spots are abundant, anemia - weakly expressed.
4. Muscle rigor. The forensic medical significance of muscle rigor is extremely great, since it helps to fix the body posture at the time of death.
This term was first proposed in 1990. V.N. Kryukov, before this the term “rigor mortis” was widely used, which did not reflect the essence of the processes taking place. The formation of muscle rigor is influenced by the following factors: individual characteristics of the body, environmental conditions, cause of death and mechanism of dying.
After death, passive movements in the joints of the limbs are easily achieved due to sharp relaxation of the muscles. But by the end of 1-2 hours after death, the skeletal muscles gradually become dense to the touch due to the contraction of muscle tissue due to its death, that is, muscle rigor develops. This process occurs in all muscles simultaneously, but ends at different times depending on the characteristics of the structure and blood supply. Since physiologically the extensors are stronger than the flexors, when examining the corpse it can be stated that the fingers are slightly bent or even bent into a fist, the arms are bent at the wrists and elbow joints, and the legs are at the knees. The muscles gradually become more dense to the touch, and at the height of the development of rigor mortis, there is no passive movement in the joints of the limbs.
If muscle rigor is disturbed during the first 24 hours, it develops again, but to a much smaller extent. Resolution of muscle rigor begins by the end of the third day, free passive movement appears in the joints of the limbs.
There is another type of muscle rigor - thermal muscle rigor. It is associated with protein coagulation in skeletal muscles, which occurs at temperatures above 50 °C. Thermal rigor rigor can also occur in cases where normal rigor rigor has already resolved and the corpse was exposed to high temperature, for example in a fire.
Based on the fact that the process of muscle death occurs slowly, under the influence of electrical stimuli it actively responds with its contraction. The duration of the response to an electrical stimulus varies for different muscles: for facial muscles - up to 2 - 5 hours, for the quadriceps femoris muscle - up to 12 - 18 hours. When examining a corpse at the scene of an accident, experts use specially designed portable devices to determine the level of electrical irritability of muscles to determine how long ago death occurred.
During the first hours after death, as a result of impact with a hard blunt object in the area of the biceps brachii muscle, it is possible to obtain an idiomuscular tumor due to local contraction of the striated muscles at the site of damage. The extent of the tumor can provide additional information about the time of death.
Rigor (muscle) rigor - muscle contraction in a living person occurs as a result of the interaction of muscle protein with ATP, which is then broken down releasing a large amount of energy. This energy is used for mechanical muscle work. Relaxation is associated with the resynthesis of ATP from ADP in the presence of oxygen. In the muscles of a corpse, ATP breakdown and muscle contraction gradually occur, and because there is no oxygen, resitis does not occur and the muscles do not relax.
Rigor mortis is intense in case of poisoning with strychnine, cicutotoxin, acids, and so on; weakly - hemolytic poisons, drugs, and so on. With asphyxia - faster due to convulsions. At high temperatures it develops and resolves faster, because biochemical reactions occur with the absorption of heat.
Rigor mortis develops after 3 - 4 hours, after 8 - 14 hours all muscles are in a state of rigor mortis. Allowed after 2 - 3 days.
Descending development and resolution. Rigor mortis, broken 10-12 hours after death, is not restored.
5. Autolysis - the property of biological objects to hydrolytically decompose their own structures under the action of enzymes. After death occurs, enzyme production continues for some time in individual organs and tissues. The active activity of enzymes (pepsin, trypsin, and so on) does not always stop immediately after death, and cells also disintegrate, and enzymes that are normally isolated from tissues are released. Tissue acidosis promotes increased enzyme activity.
Initially, autolysis manifests itself in organs with a high content of proteolytic enzymes (pancreas, adrenal glands, stomach, spleen, liver). There is a softening and liquefaction of organs and tissues, a violation of their structure.
Autolysis has a negative meaning, simulating intravital pathological processes. In addition, it allows you to determine the rate of dying (more pronounced with rapid death).
Conclusion
Death is the natural end of life. In medical practice, the period of death is counted from the moment of final cardiac arrest and death of the cerebral cortex. But at the same time, it is known that damage to the cerebral cortex (5-8 minutes after cardiac arrest) does not at all mean the death of the entire organism. Many organs and tissues survive the moment of cardiac arrest for quite a long time and can be used in transplantation (kidneys, cartilage tissue, heart, liver, bone marrow, skin and other organs).
The first stage of dying is the preagonal state, the second is the terminal pause, then the atonal period begins, then clinical and biological death.
The time period for transition from life to death for different types of injuries is not the same. In case of injuries that are accompanied by a violation of the integrity of vital internal organs (brain, heart, spinal cord), as well as with various types of asphyxia, death occurs in a short period of time, calculated from several seconds to several minutes. In forensic medical practice, this type of death is called “acute.”
As a rule, the onset of “acute” death is usually associated with primary respiratory arrest. During external and internal examination of the corpse in such cases, abundant cadaveric spots of a diffuse nature are found, occupying more than 0.5 of the entire surface of the body, ecchymosis (punctate hemorrhages) in the mucous membrane of the eyelids, cerebral edema, congestion of the internal organs, dark liquid blood in the cavities of the heart and large vessels, acute pulmonary emphysema with foci of edema, swelling of the gall bladder bed.
If the moment of cardiac arrest is preceded by an atonal period, which can last from several tens of minutes to several hours, then the resulting disorder of blood circulation leads to congestion. When examining a corpse in such cases, they find abundant, diffuse cadaveric spots, relaxation of the sphincters, pronounced swelling of the tissue of the lungs and membranes of the brain, congestive venous congestion of the internal organs, in the cavities of the heart and large vessels, dark red and yellow blood clots (fibrin).
Depending on the cause in forensic medicine, it is customary to distinguish the category, type and type of death.
Violent death means premature death, which occurred from the consequences of various influences of environmental factors (mechanical, electrical, chemical, etc.).
The type of death should be understood as a set of factors that caused the death of a person under their influence. Death can occur as a result of poisoning, extreme temperatures, hypoxic conditions arising from external causes (drowning, hanging, etc.). These types of deaths are considered under the category of violent deaths. In the category of non-violent death, the type of death is sudden death.
In forensic medicine, the type of sudden death means death that occurs as a result of hidden or even asymptomatic diseases, in the midst of visible, apparent health. Such a death is unexpected for others and raises suspicion of a violent death (for example, poisoning).
In the category of violent death, the type of death means murder (taking the life of one person by another), suicide (taking the life of oneself) or death due to a combination of unfavorable, unforeseen circumstances - an accident.
The responsibility of a forensic medical expert is only to establish the category and type of death, and establishing the type of death is the prerogative of the forensic investigative authorities, since the doctor does not have special (medical) methods for establishing the intent of the act.
The first step of a medical examiner when examining a body at a crime scene is to determine whether there are signs of life or the absence thereof. To do this, the doctor uses orienting signs of death, which include the absence of reflexes from the cornea and pupils, the absence of breathing, heartbeat, and pulse in large blood vessels.
If there are signs of life in the victim, the doctor must begin resuscitation measures and, with the help of the investigative authorities, organize the evacuation of the victim to the nearest medical facility, while he himself remains to continue examining the scene of the incident.
To ascertain death when examining a body at the scene of an incident, the doctor uses, in addition to orienting signs, reliable signs of death that develop in the corpse in connection with the onset of biological death and the development of post-mortem changes in the corpse.
Bibliography
1. Textbook "Forensic Medicine" ed. prof. Tomilina.
2. Forensic medicine" Smolyaninov (for medical universities).
3. Directory for lawyers "Forensic medical examination" Prof. Tomilin V.V.
4. Course of lectures on Forensic Medicine" by Prof. Gromov.
5. Vinogradov “Forensic Medicine” (for lawyers) M: 1991
6. A.A. Solokhin “Qualification tests in forensic medicine” M: 1994,
The concept and types of death, its main causes and factors, external and internal. Signs of violent death, medical examination, types. Patterns of the appearance and development of post-mortem changes, features of their use in forensic medicine.
presentation, added 11/27/2014
Sequence of examination of the corpse. Place, position and posture of the corpse. Objects on the corpse and in its immediate vicinity. Description of cadaveric changes upon detection of gunshot wounds. Murders for sexual reasons and using sharp objects.
test, added 06/20/2009
Studying the prerequisites for changes in the sources and system of law. Review of major changes in civil and commercial law: subjects of law, antitrust legislation, property rights, innovations in the law of obligations. Changes in criminal law.
abstract, added 05/25/2010
Asphyxia due to restriction of respiratory movements of the chest and diaphragm. The main morphological changes of the corpse, characteristic of compression asphyxia. Death from mechanical strangulation. The severity of asphyxia and the speed of death.
abstract, added 08/27/2015
The onset of biological death. Legal assessment of death. Personal non-property rights and intangible benefits that belonged to the deceased. Death as a legal fact. Death of a party during civil proceedings.
abstract, added 03/03/2009
Asphyxia: concept and classification. Three main types of compression of the neck organs: hanging, noose strangulation, manual strangulation. Compression asphyxia, its symptoms. Changes on the corpse during suffocation. General asphyxial signs during external examination of a corpse.
abstract, added 11/29/2013
The essence of the state and the institutional structure of its economy. The relationship between institutional changes and their mechanisms. Diversity of main types and causes of institutional change. The mechanism of dependence on the trajectory of previous development.
course work, added 08/22/2014
The importance of forensic medicine. Study of corpses of newborn children. Signs of extrauterine life of a child. Features of the study of corpses in cases of sudden death. Causes of sudden death in people of different ages. Study of dismembered corpses.
test, added 03/01/2009
Definition of the concept of financial legislation. Study of the main legislative changes that came into force in 2012. Consideration of features in the field of payment of taxes, insurance, accounting. Legal basis for cash transactions.
abstract, added 01/22/2015
Characteristics of the main periods of existence of the Frankish Carolingian Empire - its emergence, prosperity and collapse. Consideration of the state organization and features of the legislation of the empire. The main consequences of the Verdun division of the state.
Forensic examination of corpses: lecture
bibliographic description:
Forensic medical examination of corpses: lecture / Kan V.B., Belikov I.E. — 2002.
html code:
/ Kan V.B., Belikov I.E. — 2002.
embed code for forum:
Forensic medical examination of corpses: lecture / Kan V.B., Belikov I.E. — 2002.
wiki:
/ Kan V.B., Belikov I.E. — 2002.
Lecture IV. FORENSIC MEDICAL RESEARCH OF CORDS
Literature:
A dead human body is a rather complex object of forensic medicine. In order to effectively resolve issues of interest to law enforcement agencies in cases of discovery of corpses, forensic doctors, based on data from other biomedical sciences and their own research, have developed a theory of the process of dying and death. Based on this theory, a system of practical research of corpses at the places where they were found and in the morgue was built. The fundamentals of science and practice of this branch of forensic medicine are presented in this part of the lecture course.
The concept of death is directly related to the concept of life; life ends with death. Therefore, to understand what death is and how it occurs, it is necessary to first define life.
The most general and brief biological and philosophical definition of life is as follows: “Life is the form of existence of protein molecules.” Of the generally accepted definitions of death, attention should be paid to the one proposed by the United Nations: “Death is the complete cessation of all vital functions of the body.”
Ordinary dying, so to speak, consists of several stages that successively replace each other.
From the moment of clinical death, post-mortem changes in the human body begin to develop, which are caused by the cessation of the functions of the body as a biological system. They exist in parallel with ongoing life processes in individual tissues.
1.5-2 hours after death, fairly clear signs of post-mortem changes appear on the corpse, such as cadaveric spots, rigor mortis, rigor desiccation. Somewhat later, a significant decrease in body temperature is clearly detected, which also reliably indicates the occurrence of death.
Death classification. As already noted, death can occur from various external and internal causes. Based on the characteristics of the factors causing death, several forensic classifications of death have been created, which naturally take into account the interests of law enforcement agencies and the provisions of the criminal procedure law.
Let's consider one of the most common classifications. According to this classification, death is divided into two categories: violent And nonviolent. Violent It is generally accepted that death occurs as a result of the action of an external factor on the human body: mechanical, chemical, physical, etc.
Nonviolent death is caused by diseases and, less often, by profound age-related changes (from old age).
In some cases, the action of external and internal factors occurs together, and it can be difficult to determine which of them plays the leading role.
Violent death may be murder, suicide or accident, it is called born of violent death. Determining the type of violent death is the responsibility of law enforcement agencies; forensic doctors do not determine the type of death. But by their examination of the corpse at the scene and in the morgue, as well as examination of traces of biological origin, they can give the investigator grounds to establish the type of violent death: murder, suicide or accident. Naturally, the investigator makes the final decision based on the totality of all the data he has collected, including forensic data.
Among the possible options for non-violent death, the concept is distinguished sudden death. Sudden death refers to the death of a person, which occurred unexpectedly for those around him against the background of apparent health.
Kind of death determined by the nature of the factor that led a person to death. In this case, factors are grouped according to their mechanism of action and other characteristics.
The following types of violent death are distinguished: from mechanical damage; from mechanical asphyxia; from poisoning; from high and low temperatures; from the action of electricity; from the effects of changes in barometric pressure; from the action of radiant energy. Some other types of violent death are less common.
Violent death of the same type can be of different types, i.e. It could be murder, suicide, or an accident. Let us illustrate this with the following simple example. Let's say a person was poisoned with methyl alcohol - a strong poison. Forensic doctors, under certain circumstances, can easily establish that methyl alcohol poisoning occurred, therefore, the death is classified as violent, the type of death is poisoning. But establishing the type of death is the responsibility of law enforcement agencies. A person could consciously pour methyl alcohol into a glass and drink it, wanting to end his life. Having established this, law enforcement agencies classify the event as suicide. If it is established that the poison was poured into the glass by another person who knew what he was doing, then this is already murder. If the victim drank methyl alcohol by mistake, mistaking it for ethyl alcohol, and this mistake was not rigged by anyone, then there is an accident. When determining the type of death in the situation described, forensic medicine can practically do nothing to help the investigation. But in many cases, its help can be, if not decisive, then significant.
Non-violent death is divided into the following main types: from diseases of the cardiovascular system; from respiratory diseases; from diseases of the central nervous system; from diseases of the digestive system, etc.
The study of cadaveric phenomena allows us to solve a number of very important questions that clarify the circumstances of death, namely: when death occurred, whether the initial position of the corpse changed. Some options for the development of post-mortem processes on a corpse can provide preliminary information about the causes of death.
Post-mortem processes developing on a corpse, in their biological essence, can be divided into three large groups.
The appearance and development of cadaveric phenomena is influenced by many external and internal factors. Knowledge of their influence on the processes of post-mortem changes in a corpse is necessary, since without such knowledge it is almost impossible to use the dynamics of post-mortem processes to solve forensic and, accordingly, investigative problems.
The main internal factors of this plan are: the degree of fatness, age, the presence of serious chronic or acute diseases, the degree of alcoholization of the body and some others. These processes are significantly influenced by the cause of death and accompanying phenomena, such as blood loss, duration and severity of the agonal period, etc. The nature of clothing matters. External conditions that influence the development of post-mortem processes include ambient temperature, humidity, and the development of flora and fauna of the environment.
The nature and degree of influence of the factors listed above will be presented when describing specific post-mortem processes.
Cadaveric spots - areas of body tissue posthumously soaked in blood. Outwardly, they look like large area bruises. The color of cadaveric spots, violet-bluish or purple-blue, depends on many reasons, primarily on the color of the blood and its quantity.
Immediately after death, the skin of a human corpse is pale, perhaps with a slight grayish tint. Immediately after death, body tissues still consume oxygen from the blood, and therefore all blood in the circulatory system becomes venous. Cadaveric spots are formed due to the fact that after circulatory arrest, the blood contained in the circulatory system, under the influence of gravity, gradually descends into the underlying parts of the body, overflowing mainly the venous part of the bloodstream. Blood shining through the skin gives it a characteristic color.
To solve the issues of how long ago death occurred, the movement of the corpse, and others, it is necessary to understand the development processes of cadaveric spots. Cadaveric spots go through three stages in their development: hypostasis, diffusion and imbibition.
Hypostasis- the stage at which blood descends into the underlying parts of the body, overflowing their vascular bed. This stage begins immediately after circulatory arrest, and the first signs of coloration of the skin can be observed within 30 minutes, if there was no blood loss and the blood in the corpse is liquid. Clearly cadaveric spots appear 2-4 hours after death.
To determine the stage of development of cadaveric spots, the following technique is used: press on the cadaveric spot; if at the point of pressure the cadaveric spot completely disappears or at least turns pale, then measure the time after which the original color is restored. The fact of change (non-change) in the color of the cadaveric spot and the time of its restoration are the criteria by which the stage of development of cadaveric spots and, accordingly, the time of death are determined.
Cadaveric spots in the stage of hypostasis completely disappear when pressed due to the fact that the blood only fills the vessels and easily moves through them. After the pressure stops, blood fills the vessels again after some time, and the cadaveric spots are completely restored. When the position of the corpse changes at this stage of development of cadaveric spots, they completely move to new places, in accordance with which parts of the body have become underlying. The hypostasis stage lasts on average 12-14 hours.
Diffusion stage- the next stage of the formation of cadaveric spots, it is also called the stasis stage. As a rule, pronounced manifestations characteristic of this stage are noted 12 hours after death. At this stage, the overstretched walls of the vessels become more permeable, and an exchange of fluids begins through them, which is uncharacteristic of a living organism.
Lymph and intercellular fluid gradually penetrate through the walls of blood vessels into them and mix with the blood, they contribute to hemolysis(disintegration, dissolution) of red blood cells. The liquid part of the blood also penetrates the walls of blood vessels and permeates the surrounding tissues. As a result of these processes, the blood thickens. In the diffusion stage, when pressure is applied to cadaveric spots, they do not disappear completely, but only turn pale, and after a while they restore their color.
Full development of this stage occurs within 12 to 24 hours.
When the position of the corpse changes during this period of time, the cadaveric spots partially move to those parts of the body that become underlying, and partially remain in the old place due to the saturation of the tissues surrounding the vessels. Previously formed spots become somewhat lighter than they were before the corpse was moved.
Stage of imbibition- the third stage of development of cadaveric spots. During this period, a mixture of lymph and intercellular fluid leaked from blood vessels permeates the skin, subcutaneous fat and other body tissues in the underlying sections. This process of tissue saturation with blood begins already at the end of the first day after death and completely ends after 24-36 hours from the moment of death. When you press on a cadaveric spot that is in the stage of imbibition, it does not turn pale. Thus, if more than a day has passed since the death of a person, then when such a corpse is moved, the cadaveric spots do not change their location.
The division of the process of changing cadaveric spots into stages is quite arbitrary, since these phases do not have clear boundaries, especially at the borderline moments of time around 12 and 24 hours after death, when processes characteristic of both the previous phase and the subsequent one occur simultaneously.
As mentioned above, a variety of information can be obtained from cadaveric spots. In particular, the unusual color of cadaveric spots may indicate the cause of death. If a person died with significant blood loss, then the cadaveric spots will be very weakly expressed. When dying from carbon monoxide poisoning, they are bright, red due to the large amount of carboxyhemoglobin; when exposed to cyanide, they are cherry red; when poisoning with methemoglobin-forming poisons, such as nitrites, cadaveric spots have a grayish-brown color. On corpses in water or a damp place, the epidermis loosens, oxygen penetrates through it and combines with hemoglobin, this causes the pinkish-red tint of corpse spots along their periphery.
Changes similar to those that occur at the surface of the skin also occur in the internal organs; these changes are studied during the opening of body cavities and internal organs. It should be noted that cadaveric spots in the head area, especially the scalp, can be mistaken for a hematoma.
Sometimes, against the background of cadaveric spots, post-mortem hemorrhages, called by doctors, can be found ecchymoses. Externally, they look like rounded areas, slightly protruding above the surface of the skin, up to 5x5 mm in size, and usually appear 5-6 hours after death. They are more typical for the corpses of young people who died from drowning in water, from hanging in a noose, from alcohol poisoning, etc. They should not be confused with intravital hemorrhages.
In those places where the skin of the corpse was in close contact with hard protruding areas of the surface on which it was located, the relief of this surface is clearly visible in the form of whitish areas of skin that are not soaked in blood. In the practice of forensic medicine, there are cases where, based on such patterns on cadaveric spots, the surface on which the corpse was located at the time of the formation of cadaveric spots was identified.
As noted above, one of the main methods for studying cadaveric spots is the method of applying pressure to the cadaveric spot. Pressure is usually applied in the interscapular or lumbar areas, retreating 2-3 cm from the midline. If a corpse is found in a position other than on the back, the most underlying areas of the cadaveric spots are examined. The pressure is produced by a special dynamometer, and in its absence, by the palmar surface of the nail phalanx of the index finger. In this case, the pressure force should be 2 kg per 1 sq. cm, pressure duration 3 seconds. These conditions must be strictly observed, since failure to comply will lead to an error in the calculations. The time of restoration of the color of the cadaveric spot is recorded using a stopwatch. After pressing on the cadaveric spot, the corpse must be rotated so that the place of pressure takes its original position, i.e. one in which a cadaveric spot was formed.
Assessing cadaveric spots over time, taking into account external and internal conditions influencing the development of this post-mortem phenomenon, allows us to solve a number of forensic issues.
Rigor mortis. Rigor mortis is usually called a condition of the muscles of a corpse, in which they become denser and fix parts of the corpse in a certain position. A numb dead body seems to become stiff.
Immediately after death, all the muscles of the human body relax, lose their inherent elasticity during life, the face takes on a calm appearance, which is probably where the word deceased comes from.
The process of rigor mortis develops simultaneously in all skeletal and smooth muscle muscles. But its manifestation occurs in stages: first in small muscles - on the face, neck, hands and feet, then rigor becomes noticeable in large muscles and muscle groups. Pronounced signs of rigor are observed 2-4 hours after death. The increase in rigor mortis occurs up to 10-12 hours from the moment of death. For about 12 more hours, rigor remains at the same level. Then it starts to disappear. Forensic scientists use the term resolution of rigor mortis to denote the process of gradual disappearance of rigor of the muscles of a corpse.
Rigor mortis is assessed by forensic doctors during external examination at the place where the corpse was found and in the morgue. The assessment is made using a three-point system (weak, moderate, good) sequentially in each muscle group. The principle of uneven manifestation of rigor mortis in large, medium and small muscles is the basis for determining the duration of death by rigor mortis.
Rigor mortis can be resolved (broken) artificially by applying physical effort (for example, bending and straightening the numb limb). If rigor mortis is affected in this way within a period of up to 8-10 hours from the moment of death, then rigor mortis will be partially restored in the future in the disturbed muscles. In cases where rigor mortis is exposed after this period of time, it does not recover. This pattern is used to resolve the issue of possible movement of the corpse.
Rigor mortis develops not only in skeletal muscles, but also in the smooth muscles of internal organs. As a result, some post-mortem processes occur in the internal organs, which must be taken into account when examining corpses. Immediately after stopping, the heart is in a relaxed state, then, as muscle rigor increases, its muscles tense, especially in those parts where it is more pronounced, for example, in the left ventricle, blood is squeezed out of the cavities of the heart under the influence of contracting muscles. With painful changes in the myocardium, the heart muscles almost do not stiffen. Post-mortem changes associated with the formation of rigor mortis also occur in other internal organs.
The process of development of rigor mortis is significantly influenced by various external and internal factors. At elevated ambient temperatures (above +25° C), rigor mortis develops faster; accordingly, at lower temperatures this process slows down. Rigor rigor grows faster in dry air, and slower in humid air. In persons with developed muscles, rigor mortis grows faster and reaches greater severity, and, conversely, in children, old people, emaciated and sick people, this cadaveric phenomenon forms slowly and is less pronounced. Rigor mortis develops more strongly with injuries and burns, large loss of blood, diseases of cholera, tetanus, and epilepsy. All these factors must be taken into account to avoid erroneous conclusions from the results of a rigor mortis study. These factors have the opposite effect on the resolution of rigor mortis. For example, at low temperatures, rigor develops more slowly, but also lasts longer; at elevated temperatures, it forms faster, but also resolves faster.
A muscle condition similar to rigor occurs when a corpse is exposed to elevated temperatures (more than 50°-60° C). In muscles exposed to heat, proteins, and along with them muscle fibers, contract, leading to muscle tension. And since the flexor muscle groups are more powerful than the extensor ones, the corpse as a whole takes on a characteristic pose, called the boxer’s pose.
The study of muscle rigor during an external examination of a corpse at the place of its discovery and in the morgue allows one to obtain information for solving the following important problems.
Cooling the corpse. Normally, in a living person, the body temperature, measured in the armpit, ranges from +36.4° to +36.9° C. In the internal organs and tissues of the body, the temperature is 0.3-0.5 degrees higher. Constant temperature is ensured by thermoregulation processes. These processes stop after the regulatory activity of the central nervous system stops, and the temperature begins to decrease, trying to equalize the ambient temperature. However, it should be remembered that the body temperature at the time of death of a person can be higher than the specified norm by 1°, 2° and even 3° C due to infectious diseases, poisoning, overheating of the body and similar processes. In addition, according to some researchers, the temperature of a corpse can increase immediately after death by 1°-3° C. According to literature data, an increased body temperature of corpses in the first hour after death is observed in approximately 15% of cases.
Naturally, the rate of cooling of a corpse depends on many external and internal factors. First of all, it depends on the ambient temperature. The lower it is, the more intense the cooling of the corpse. If the ambient temperature is higher than body temperature, the corpse will not cool down at all. Air humidity also affects the cooling process; in a damp, cold environment, cooling is more intense. The presence and condition of clothing plays a big role. The temperature, thermal conductivity and heat capacity of the substance on the surface of which the corpse is located are important. Ventilation of the room, exposure to direct sunlight, etc. play a role.
Of the internal factors, the most important are: fatness (development of subcutaneous fat), massiveness and size, age (children's corpses and the corpses of elderly people cool faster). People who are exhausted and weakened by the disease, who have lost a lot of blood, lose their temperature more intensely after death.
It must be remembered that when a person is in sub-zero temperatures, the surface parts of the body can be significantly cooled, “icy” to the touch, while the temperature inside the person’s body will be quite high.
Thus, by studying the process of cooling a corpse, one can obtain useful information for solving a number of issues.
Corpse desiccation. Immediately after death, the process of cadaveric desiccation begins. From the most moistened and unprotected areas of the body surface, liquid evaporation begins, which leads to drying and thickening of the tissue, these areas of the tissue darken. Such areas of the body are those in which the epidermis is damaged - the surface layer of the skin, as well as the surfaces of the mucous membranes exposed to the external environment, areas of transition from the mucous membranes to the skin, areas of loose epidermis, areas of the epidermis affected by certain skin pathologies. Specifically: the first to dry out on a corpse are the intravital and postmortem injuries, the eyeballs, the scrotum and head of the penis in men, the labia in women, the area of the red border of the lips, the tip of the tongue protruding from the mouth, and later the tip of the nose, ears, fingertips and etc.
The time characteristics of the appearance of drying out depend primarily on the temperature of the air surrounding the corpse and humidity. Under normal room conditions, drying becomes noticeable after 2-3 hours on the corneas and white membranes of the eyes, if they are open. Drying of the corneas looks like clouding; such changes are called “Larchet spots.” After 6-12 hours, the exposed areas of the eyeballs become yellowish-gray.
In windy, dry weather, outdoors, the first signs of clouding of the corneas of open eyes are observed within an hour after death.
Under appropriate conditions, the drying process of newborn corpses occurs very quickly. According to some authors, up to 100 grams of liquid per day can evaporate from such a corpse, which can be very noticeable on a small body.
Areas of the epidermis damaged postmortem (so-called parchment spots), as well as areas around the red border of the lips, areas of pathologically altered epidermis after drying can have a reddish-brown color, thereby simulating intravital damage. However, upon careful examination of such areas of skin, differences are easily detected.
The process of drying a corpse can continue until almost complete evaporation of moisture from it, in this case they speak of mummification of the corpse. This phenomenon will be discussed below.
Signs of cadaveric desiccation are analyzed by forensic scientists to determine the time of death, as well as for other purposes.
Cadaveric autolysis. Cadaveric autolysis, like previous postmortem changes, is considered by most authors to be an early cadaveric phenomenon; some assess this phenomenon as a supravital reaction. The essence of the process is that disorganized tissue enzymes after death continue their effect on surrounding structures, destroying them to one degree or another. Signs of enzyme exposure are found mainly during autopsy. Based on them, as well as on other cadaveric phenomena, the question of how long ago death occurred is decided.
The second group of phenomena studied on a corpse in order to determine the duration of death are phenomena associated with the survival of individual tissues of the body. After the death of the organism as a whole, individual tissues are still able to exhibit their functions. To determine the time of death, the ability of these tissues to react in response to a particular irritation is used. In particular, muscles contract in response to electrical or mechanical stimulation, and some tissues respond to chemicals. Such tissue reactions are called supravital.
Muscle response to electrical stimulation. If needle electrodes are inserted into the opposite ends of any muscle of a corpse, for example the biceps, and voltage is applied, then a fresh corpse will experience contraction of this muscle to one degree or another. The force of contraction is assessed on a three-point scale. A strong contraction is observed up to 2-2.5 hours after death, an average contraction up to 2-4 hours, a weak contraction up to 4-6 hours after death. The technique requires compliance with certain conditions: the use of a current of a certain voltage and strength. The good thing about the technique is that the influence of external conditions on its results is insignificant.
Muscle response to mechanical stress. When struck by a hard object with a limited striking surface, for example, a metal stick, a swelling is formed on a muscle (say, the biceps) of a fresh corpse, which is called an “ideomuscular tumor.” The presence of such a muscle reaction to mechanical impact indicates that a short time has passed since death. Visually, such a reaction can be detected within a period of up to 6 hours from the moment of death. In the period from 6 to 11 hours, the reaction can only be detected by feeling (palpating) the site of impact. At a later date, the reaction to the impact will be negative, which will be reflected in the formation of an indentation at the site of the impact. External conditions and the cause of death do not have a significant impact on this reaction.
On fresh corpses, muscles react to mechanical irritation of tendons. When a tendon is struck, the corresponding muscles contract. This looks similar to how neurologists test tendon reflexes in patients by tapping their knees and Achilles tendons. A positive reaction to tapping on all tendons indicates that no more than 1.5-2 hours have passed since death. If only some muscles reacted positively, then about 6-8 hours have passed.
The reaction of the pupils to the administration of atropine and pilocarpine. After death occurs, under the influence of internal biomechanisms, the pupils of the eyes dilate, then narrow for about 2 hours, then dilate again.
The pupils react to the administration of atropine and pilocarpine (as well as some other chemicals), dilating or contracting, and the strength of the reaction is inversely proportional to the time of death, which is used to determine the time of death. In the period up to 11 hours after death, a double reaction is observed, namely, from the injection of atropine, the pupil dilates, and after the injection of pilocarpine it narrows. A separate reaction (narrowing or expansion) is detected on average up to 24 hours from the moment of death. After 24 hours, the pupils do not respond to the administration of atropine and pilocarpine.
In addition to the early cadaveric changes and tissue survival phenomena described in the previous section, a number of processes develop on the corpse, which differ from the first two groups in their later appearance, which is why they were called late cadaveric phenomena.
Late cadaveric phenomena include: rotting, mummification, skeletonization, fat wax, peat tanning, as well as damage to corpses by animals and plants.
In general, all late cadaveric phenomena are characterized by a strong dependence on the conditions of the corpse’s location and a large scatter in the time characteristics of their occurrence, which significantly complicates their use for solving forensic medical issues.
All late cadaveric phenomena, to a certain extent, can be divided into two groups: first - destructive, second - preservative. On one corpse, different cadaveric phenomena can simultaneously develop, for example, mummification and rotting, if parts of the corpse are in different conditions.
Rotting. Rotting belongs to the group of destructive cadaveric phenomena. It develops as a result of exposure to microorganisms on the tissues of a corpse. Under their influence, tissues are destroyed into simpler biochemical and chemical components. As a result of the formation of substances such as ammonia, hydrogen sulfide, methyl mercaptan, ethyl mercaptan and some others, a characteristic putrid-cadaverous odor appears.
Putrefactive bacteria are common inhabitants of the human intestine. There they (during human life) are in balance with other microorganisms and vital processes of the body, perform their functions and, under normal conditions, do not go beyond the boundaries of their distribution areas. After the death of a person, everything changes: many types of putrefactive bacteria begin to uncontrollably multiply and spread in the human body, this leads to decay of the corpse.
Initially, putrefaction develops most strongly in the large intestine, this is accompanied by the formation of a large amount of gases, which accumulate in the abdomen. Intestinal bloating can be noted within 6-12 hours after a person’s death. Then signs of decay appear in the form of a dirty green color, first in the right iliac region, then in the left. This coloring occurs due to the formation of sulfhemoglobin from blood hemoglobin and released hydrogen sulfide. Under room conditions, putrefactive staining appears in the iliac areas on the anterior abdominal wall by the end of the second day. The rot then spreads through the blood vessels, mainly veins, to other areas of the body. This process is accompanied by the appearance of the so-called putrefactive venous network - a clearly visible dirty green pattern of veins. Signs of a putrefactive venous network are observed 3-4 days after death.
Also, on the 3-4th day of the development of putrefaction, an increase in the accumulation of putrefactive gases in the subcutaneous fat and other tissues is noted. Due to this, the corpse bloats, the so-called putrefactive emphysema. Body parts increase sharply in size: abdomen, chest, limbs, neck, nose, lips, in men - the scrotum and penis, in women - mammary glands. Bloody discharge is observed from the natural orifices of the body; this should be differentiated from the manifestation of injury. After 4-5 days, blisters appear on the surface of the skin due to its delamination, filled with a foul-smelling reddish-brown putrefactive liquid. Partially exfoliated epidermis can be displaced due to mechanical action, and the reddish dermis, the underlying layer of skin, becomes visible. Such manifestations of rotting mimic skin burns. On days 6-10, the epidermis completely peels off and can be easily removed along with nails and hair. Subsequently, through the damaged areas of the skin, the accumulated and newly released putrefactive gases leave the corpse, the size of the corpse and its parts decreases. The processes of decay soften and disorganize tissues - the so-called putrid melting of a corpse. As a result, the bones are exposed in places, especially in places where they are covered with a small amount of soft tissue. Complete putrefactive decay of the soft tissues of a corpse (skin, fatty tissue, muscles, some components of internal organs, etc.) under conditions suitable for decay can occur in 3-4 weeks. After this period, bones, ligaments, cartilage, and formations consisting of a large amount of connective tissue are preserved.
A corpse in a state of significant putrefactive changes is a very unpleasant sight. The presence of putrefactive tissue destruction, their greenish-dirty color, and fetid odor create the basis for a negative assessment of the possibilities of productive forensic research of such corpses. It seems that it is impossible to establish the cause of death, the mechanism of its occurrence and resolve other issues regarding such a corpse. However, this is not always the case. On putrefactively altered corpses, it is possible to detect and determine damage, traces, some well-defined pathological processes, for example, cardiosclerosis, atherosclerosis, etc. Therefore, any degree of putrefactive decomposition of a corpse is not a basis for refusing to order and conduct a forensic medical examination of the corpse.
Skeletonization. In the absence of natural and artificially created processes preserving the corpse, such as mummification, fat wax, peat tanning, exposure to salt solutions, freezing, etc., the process of decay turns into the process of skeletonization. The essence of this post-mortem phenomenon is that through putrefactive melting and as a result of the eating of the tissues of the corpse by insects, the soft tissues of the corpse completely disappear from the bone base. Clearly visible signs of skeletonization can be noted on the corpse after 1 month of the corpse being in appropriate conditions. Almost complete skeletonization (only bones, ligaments and cartilage remain) can occur in 3-6 months, and after a year the skeleton disintegrates into individual bones, as most of the ligamentous apparatus is destroyed.
Conditions that accelerate the decay process naturally accelerate the skeletonization process. However, the greatest importance for the complete cleansing of skeletal bones from soft tissues is the presence of a large number of insects and other types of animal carrion eaters, complementing and replacing each other in the destruction of the soft tissues of the corpse.
Of the insects, the most active in this regard are flies and beetles of several species. Rodents, in particular rats, destroy the soft tissues of a corpse at the initial stage of decay and even before its signs appear. Parts of the corpse can be chewed by wolves, jackals, cats and dogs. There have been cases of birds damaging corpses. The intense impact of animals on a corpse accelerates its skeletonization.
In an aquatic environment, a corpse can be actively eaten by aquatic animals, primarily various crustaceans, as well as fish.
Plants growing in Russian latitudes usually do not have a significant effect on the corpse. Only the development of certain types of mold is noted on the corpse, and when the corpse is in the open ground, some plants can grow through it. The study of plants in the bed of a corpse sometimes makes it possible to determine how long ago it was located at the place of discovery.
Under certain conditions where a corpse is located, its tissues are subject to the preservative influence of environmental factors.
Mummification. Mummification is the process of post-mortem changes in the tissues of a corpse, during which moisture almost completely evaporates from them. In this case, the tissues become denser, decrease in volume, the weight of a completely mummified corpse is no more than one tenth of the original one.
For the development of mummification, a number of conditions are necessary, in particular: good ventilation of the location of the corpse; high temperature, although mummification can also take place at room temperature under conditions of very good ventilation and dry air; low air humidity. Under the most favorable conditions, complete mummification of a human corpse of average build can occur in 4-6 months, while the average time for complete mummification is indicated by different authors within 6-12 months. Partial mummification can be detected on corpses after 1-2 months. The corpses of children and people with a low content of subcutaneous fat mummify faster than others.
Under appropriate conditions, mummified corpses can be preserved indefinitely without undergoing changes, so determining the age of death from a corpse whose mummification has ended is extremely difficult.
It should be noted that forensic medical examination of mummified corpses makes it possible to resolve a number of issues related to the occurrence of death. In particular, dried corpses retain signs of damage, traces of imposition, and some traces of painful changes in organs and tissues. Therefore, such corpses can and should be carefully examined.
Fat wax. Fat wax is a cadaveric change related to late cadaveric phenomena of the preservative type; its second name is saponification. The main conditions for the formation of fat wax are high humidity in the environment where the corpse is located and minimal air access. Saponification develops in water, in dense and moist soils and in other similar conditions.
The essence of the process is the gradual decomposition of the fat contained in the corpse and the washing out of some of the resulting derivatives. The remaining water-insoluble fatty acids combine with alkali and alkaline earth metal salts, forming a substance called fat wax. Depending on which metal salts the fatty acids are combined with, the fat wax can be either a gelatinous substance of a dirty gray color or a dense substance of gray-white color with a greasy sheen.
Various authors indicate that they observed the first signs of saponification of the tissues of a corpse from 25 days to 3 months after death. Complete saponification of a corpse occurs no earlier than 6-12 months on the corpses of adults; on the corpses of children it is possible a little faster.
The study of saponification processes only tentatively allows us to speak about the duration of death.
Peat tanning. Peat tanning is a preserving late cadaveric phenomenon, the essence of which is the tanning (compaction) of tissue under the influence of an acidic environment. In forensic medical practice, corpses that have undergone such a change are even less common than corpses in a fat wax state. Mostly such finds were made in peat bogs, where body tissues of deceased people were exposed to long-term exposure to humic acids. Under the influence of these acids, the skin of corpses and internal organs become denser and acquire a dark color. Under the influence of acids, calcium is washed out of the bones and they become soft and flexible. Peat-tanned corpses last a very long time. It is possible to detect and study damage on such corpses.
Various authors have included several more post-mortem processes in the group of preservative cadaveric changes. Salting corpses - a phenomenon in which concentrated solutions of salts or salts in dry form act on a corpse; by their influence they stop the processes that destroy the corpse. There is literature data indicating the possibility preservation of corpses when they get into oil. Formalin, some alcohols and other chemicals have a preservative effect on biological tissues. Low temperature- one of the factors that can preserve corpses unchanged for a long time. The corpses of prehistoric animals are known to have been preserved to this day in permafrost.
The conditions under which the corpse is located from the moment of death until the moment of its examination may change. And then, instead of some post-mortem processes, others begin to develop. In practice, there are common cases when different conditions simultaneously act on a corpse and, accordingly, its different parts change differently. For example, a corpse located on the soil, on the ground side, rots and is destroyed by corpse-eating insects, and at this time the parts of the body facing upward are mummified due to ventilation and drying.
If a corpse with signs of rotting begins is placed in a dry, well-ventilated place, then the decay processes are suspended and mummification develops. The decay process also stops when the ambient temperature drops below 0° C. Conversely, a corpse preserved in some way, for example, frozen in the cold season, can begin to rot and be destroyed by animals when it warms up.
Determining the time of death is of great importance for establishing the circumstances of the death of a person who died in conditions of non-obviousness. Such information is even more significant when solving and investigating murders.
Time of death a person can be recognized in different ways. It may be indicated by elements of the situation at the place where the corpse was discovered, witness testimony, etc. However, in any case, both in the absence of any information and in its presence, a forensic medical determination of how long ago the death occurred must be carried out.
When working with corpses that do not show signs of decay, i.e. When examining fresh corpses, forensic methods for determining the duration of death should be applied as early as possible, immediately at the place where the corpse was discovered. This must be done because the accuracy of establishing the duration of death is higher, the less time has passed since death. For example, if you determine the time of death 2-3 hours after its occurrence (which is realistic when examining a corpse at the place of its discovery), then you can establish it with an accuracy of 20-30 minutes, and if you do this after 1-2 days (when examining corpse in the morgue), then the accuracy at best will be 8-10 hours. It is quite obvious that with the first answer, it is much easier to solve and investigate a crime than with the second.
Possibility of establishing the time of burial of a corpse. Investigative authorities in the process of work have to deal with two possible options for studying buried corpses. The first is that the corpse is buried officially, in a coffin; the time of its burial and the events preceding it are known; in such cases, as a rule, there is no need to determine the age of burial. The second option is that the corpse was buried secretly, is in the ground without a coffin, the time of its burial is unknown or known only approximately and requires identification.
Let us consider the process of post-mortem changes in a corpse in relation to the second version of investigative situations. As in the study of corpses located on the surface of the earth, the age of burial is determined by the dynamics of post-mortem changes in the corpse.
The decomposition processes of buried corpses in most cases proceed more slowly than corpses located on the surface of the earth or indoors. This is explained by a number of reasons, among which the following are significant: a lower and more stable temperature for preserving the corpse than the temperature indoors or outdoors in the warm season, especially when the corpse is buried deeply (over 1-1.5 m); absence of most corpse-eating insects (primarily flies); slow bacterial decomposition of the corpse due to low temperature and lack of oxygen. These factors apply to all types of soils. The nature of the soil, its humidity, porosity, acidity and other features also influence the nature and rate of development of post-mortem destruction of the corpse.
The depth of the burial is of great importance. If the corpse is covered with only 20-30 cm of soil, then the intensity of its decomposition is not much different from that on the surface of the earth, and in soils with a large number of rotted and decaying plants inhabited by many insects, the post-mortem decomposition of the soft tissues of corpses can be even more intense, than on the surface of the earth, due to the high content of bacteria and the accessibility of corpse tissue to corpse-eating insects. As the depth of burial of corpses increases, the effect of these factors of corpse decomposition decreases.
Corpses buried at a depth of 1.5-2 m undergo pronounced putrefactive changes by the end of the first year, the process of skeletonization appears in the head and limbs, the lower jaw is not yet separated from the skull, the chest and stomach are sunken. Over the next 1-2 years, soft tissues are almost completely destroyed, only individual sections of them can be detected, ligaments and cartilage are mostly still preserved. After 5 years of the corpse being in the ground, the ligaments and cartilage almost completely disappear. In dry soils, after 10 years of burial, pronounced drying of the skeletal bones is observed. Further residence of the skeleton in the ground leads to a significant decrease in bone mass, their porosity and fragility increases.
Changes in corpses located in the ground allow us to only roughly judge the age of burial, therefore, in addition to purely forensic data, when resolving such an issue, it is necessary to try to obtain information from an investigative and operational plan.
Inspection of the corpse at the place of its discovery. In forensic science, the scene of an incident is a section of terrain or premises within which traces of a crime were found. The boundaries of the scene of the incident can be quite clear in cases where the events unfolded strictly in one place, for example, in the case of a crime (for example, murder) being committed in an apartment in an apartment building, the scene of the incident will be limited to the boundaries of this apartment. In large-scale incidents, such as a train or plane crash, the accident site can cover an area of tens of hectares of land.
Clear natural boundaries of the scene of the incident may not always be established; in such cases they are established artificially, for example, with a radius of two hundred meters around a corpse found in a wooded area. There may be several crime scenes in one criminal case. For example, a murder occurred in an apartment, then the corpse was taken out and hidden outside the city. In this case, we will highlight two locations of the incident. More often we encounter cases where the place where a corpse was found is the scene of an incident (crime).
Inspection of the scene of the incident - an urgent investigative action consisting in the direct perception of the territory in which a particular crime was committed, with the aim of retrospectively understanding the essence of the event that occurred, and also carried out to detect, record and seize material and other evidence as evidence of what happened.
When conducting an inspection of the crime scene, the investigator (the main person during the inspection) must obtain information of varying degrees of reliability to answer the following questions.
Answers to questions can be obtained by examining and analyzing the situation in which traces were discovered and examined, examining the corpse, by obtaining information from relatives, neighbors, witnesses and other persons, by analyzing the information received from the perspective of the experience of participants in the inspection of the scene and other methods.
In urgent cases, an inspection of the scene of the incident may be carried out before the initiation of a criminal case. In these cases, if there are grounds for it, a criminal case is initiated immediately after an inspection of the scene of the incident.
Thus, an inspection of the scene of an incident is the only investigative action for which the law makes an exception and allows it to be carried out before the initiation of a criminal case.
The procedure for carrying out the inspection is regulated: there is an indication that, if necessary, the investigator can invite a specialist of the relevant profile to participate in the inspection of the scene of the incident. However, the same article says that, if necessary, the investigator independently performs during the inspection: measurements, photography, filming (which in today’s world is equivalent to video filming), drawing up plans and diagrams, making casts and impressions of traces. The investigator can, if necessary, inspect items and documents found during the inspection of the scene of the incident directly at the scene of the incident; items that are appropriate to be seized are packed according to the appropriate rules.
The procedure for examining the scene of an incident with a corpse has been developed in relation to various situations. The inspection should be carried out methodically using one of the recommended systems.
Theoretically, there are many options, methods and techniques for inspecting the scene of an incident. The choice of one or the other depends on many circumstances. First of all, it is determined by the nature and area of the territory that is to be inspected, secondly by the nature of the crime, as well as other circumstances.
The choice of methodology for examining the scene of the incident is carried out during a general familiarization with the scene of the incident. At this stage, the investigator determines the boundaries of the crime scene and key objects. One of the key objects is a corpse. In the process of familiarizing yourself with the scene of the incident, it is advisable to take orientation and overview photographs and make a video recording. For most cases, it is considered optimal the beginning of the inspection of the crime scene from the corpse. With this inspection procedure, care must be taken to preserve traces distant from the nodal point. In most cases, it is advisable to move away from the corpse in a spiral. However, in any direction of movement during an inspection of the scene of an incident, it is necessary to observe the rule of two stages - first, a static inspection of a unit, section or the entire scene of the incident is carried out, and then a dynamic one. In the first stage, the movement of objects and their parts is excluded, in the second - objects and their parts can be moved in order to more fully examine them.
When examining a corpse at the scene of an incident, three main versions about the nature of the incident must be put forward and, if possible, verified, namely, murder, suicide, or an accident. It is unacceptable, even under the most seemingly obvious circumstances, to deliberately exclude any of these versions. Practical experience shows that, trying to reduce labor costs for inspecting the scene of an incident, the participants in the inspection, and, first of all, the investigator as the person responsible for this action, try to concentrate their efforts on working on one of these versions. In the future, if new circumstances arise that exclude the initially preferred version, the opportunity to fully carry out work on other versions will be irretrievably lost. Accordingly, the chances of qualitatively understanding what happened will be lost. It should be noted with regret that at present, when examining corpses at the scene of their discovery, law enforcement officers give preference to versions of suicide or an accident, which leads to an increase in the number of latent murders, and, accordingly, impunity for killers.
Immediately upon arrival at the scene of the incident, the forensic physician must make sure that everything necessary to save the life of the deceased has been done, and that it is no longer possible to help the deceased. Such actions of the forensic doctor are especially important in cases where there were no doctors at the scene of the incident before him. If, at the time of his arrival at the scene of the incident, there was an emergency medical team there, then the forensic physician only ascertains death, studying the presence of its reliable signs.
When examining a victim, the first thing to check is the person’s breathing and heartbeat. Breathing is most accurately determined using a phonendoscope in the area of the jugular fossa on the front surface of the neck in its lower part. The presence of cardiovascular activity is checked by palpating the pulsation in the area of the carotid arteries on the left or right side of the neck, or in the area of other large arteries lying close to the surface of the body.
As the earliest signs of death, indicating irreversible processes in the central nervous system, it is necessary to study the following: Beloglazov’s sign - when the eyeball is compressed on both sides in a dead person, the pupil changes its shape, becomes oval or slit-like instead of round, in a living person there is no such phenomenon observed; corneal and conjunctival reflexes are checked by touching the cornea of the eye with the edge of a sheet of paper or the edge of a piece of fabric, etc., while in a living person a reaction of closing the eyelids is observed, in a dead person this reaction is absent; reaction of the pupil to light - in a living person the pupil reacts to light by constriction (it is better to use a flashlight to illuminate the pupil), in a dead person the pupil does not react to light.
When people are found to be hypothermic, the above tests may be difficult to perform. In these cases, the method of determining the temperature in the rectum is indicative. A decrease in this temperature below +20° C is a reliable sign of death.
Having not identified reliable signs of death in the victim or having detected at least weak signs of life, the forensic physician who arrived at the scene of the incident is obliged to make every effort to carry out resuscitation measures, continuing them until the arrival of emergency medical services.
Immediately before examining the corpse, it is necessary to photograph it. Practice shows that it is better if the corpse is photographed by a forensic specialist with the participation of a forensic physician. In this case, photographs will be taken from the right directions and important details will not be missed. Photography should be carried out from four sides in natural light; if natural lighting is not enough, then preference should be given to photographing under lighting from constant light sources of at least two. The worst option is photographing a corpse with flash.
Before photographing a corpse, it is necessary to mark the area adjacent to it with special marking and scaling means (plates with numbers and letters, arrows, scale rulers, etc.).
In parallel with photographing, it is advisable to video record both static elements of the crime scene, including the corpse, and the dynamics of the actions of members of the investigative team in relation to these objects. Video recording of the corpse must be done from at least two sides; it is advisable that there are no unfixed surfaces of the body of the deceased person. For video shooting, you need professional-grade equipment with the ability to capture macro- and micro-objects.
According to the rules mentioned above, in responsibilities of a medical specialist in the field of forensic medicine (or medical expert) when examining the scene of an incident includes:
When examining a corpse at the place of its discovery (at the scene of the incident), the forensic physician is obliged to establish, show to the investigator and formulate verbally for recording in the protocol the following information about the corpse (given in the order in which it should be obtained when examining the corpse):
The study of post-mortem phenomena on a corpse during an inspection of the scene of an incident should be carried out twice: at the beginning and at the end of the inspection, first of all this concerns the measurement of the temperature of the corpse. In this case, it is necessary to measure the temperature of the air surrounding the corpse, and, if possible, its humidity.
Detection and removal of traces of biological origin is another important activity of the forensic scientist at the crime scene. Traces of biological origin in criminology and forensic medicine most often refer to traces of substances that originate from the human body or which are assumed to originate from a person. When searching for traces of this kind, substances originating from animals or plants, as well as derivatives of inanimate nature, similar in appearance to substances of biological origin, can be found.
More often than others, traces of blood, semen, saliva, urine, feces, vaginal discharge, hair, particles of body tissue, and other substances may be found at the scene of the incident. Corresponding animal tissues, plant particles, as well as synthetic and mineral substances may be similar to them.
At the scene of the incident there may be clearly visible traces of biological origin, most often these are traces of blood, especially in cases where the corpse has multiple injuries or damage in the area of large blood vessels. The absence of traces of blood when there are injuries on the corpse most likely indicates that the damage was caused not in this place, but in another. With a rough massive mechanical impact on the human body, multiple well-defined traces of biological origin can be formed by other human tissues.
Detecting traces of biological origin is not difficult in most cases. A careful examination of the components of the crime scene will give a complete picture of such traces. It is necessary to note their location, shape, size, relative position and location in relation to the corpse, record them in photographs and videos, mark them on the plan and describe them verbally in the protocol. If they are well captured by photo and video, their description in the protocol can be made brief.
It is not necessary to remove all visible traces, which are present in large quantities. It is advisable to take only a few of them. If the traces are large, they can be partially removed. Traces should be extracted selectively in such a way that traces of all variants of appearance from different areas of the crime scene are included for laboratory research.
Items that carry traces of biological origin and the traces themselves must be packaged after preliminary drying in room conditions. If possible, drying should be avoided on heating devices and in places exposed to direct sunlight. Placing wet traces in plastic bags, jars and similar conditions entails their intensive decay at above-zero ambient temperatures. If it is possible to place traces of biological origin in a refrigerator with a negative temperature, then decay does not develop and they remain suitable for research.
From the point of view of procedural law, the rules for packaging material evidence with traces of biological origin do not differ from those for other material evidence.
Under certain conditions, the so-called consequences can be of great importance for solving problems of investigation. negative circumstances.
In relation to working with traces of biological origin at the site of discovery of a corpse (scene of an incident), negative circumstances should be understood as the absence of traces in situations where they should have been. For example, it has already been mentioned that the absence of blood or a small amount of it in the place where a corpse was found with significant damage indicates that bleeding from the injuries did not occur at the place where the corpse was found, but in another place and, therefore, the place where the corpse was found is not, in the full sense this word, a crime scene.
When fulfilling his duties to examine the scene of the crime, the forensic physician must not violate a number of rules that are aimed at preserving, if possible, of course, the unchanged appearance of the corpse and traces of biological origin. In particular, a forensic physician at the scene of an incident does not have the right to:
Based on the results of the external examination of the corpse at the place of its discovery and the results of the process of identifying and recording traces of biological origin, the forensic physician can orally answer the following questions to the investigator.
If necessary and depending on the conditions of a particular case, the forensic physician can answer other questions of the investigator if they do not require complex additional research.
For a high-quality inspection of the place where a corpse was found, it is important not only to construct a forensically correct examination and comply with all the requirements for this investigative action, it is also important to carry it out competently from the point of view of forensic medicine and its requirements for this investigative action. One of the requirements of forensic medicine for examinations of corpses and places of their discovery is the requirement for a differentiated approach to examination in cases of different types of death. Compliance with this requirement allows you to collect information as completely as possible at the scene of the incident to resolve the issue of the causes of death and the mechanisms of influence of the external factor that led to death. Therefore, we present some features of the inspection of the scene of the incident for various types of death.
In case of damage from blunt or sharp objects: it is necessary to describe in detail the nature of the damage, the relationship of the damage with traces of biological origin; make assumptions about possible instruments of injury and try to find these instruments; it is necessary to try to guess the mechanism of causing damage and, thereby, the mechanism of interaction between the victim and the offender; try to tentatively determine the time required for the offender to cause damage and the force applied; the possibility that not one, but several criminals acted.
In case of injury from motor vehicles: it is important to carefully describe the position of the corpse, its location in relation to the vehicle or its tracks; record the condition of clothing and marks on it; presence on the vehicle of traces of interaction with the victim’s body; the presence of traces of biological origin in vehicle tracks, etc.
In case of a railway injury: it is necessary to thoroughly study and describe the position of the corpse, the location of it and its parts in relation to the railway rails, embankments and other parts of the transport route; identify traces of biological origin along the highway in both directions from the corpse, establish the distance from them to the corpse; describe the presence of marks on the clothing of the corpse, their nature, etc.
In case of aviation injury: it is very important to clearly record the location of the corpses and their parts in relation to the aircraft and its parts; establish the relative position of body parts that could presumably belong to one person; record the location of body parts that can be identified by clothing, documents, biological characteristics or other data; the relative position of corpses and parts of corpses with similar injuries; the presence and location of traces of biological origin on parts of the aircraft and other features in accordance with the specific situation.
When falling from a height: it is necessary to record the position of the corpse and its location relative to the object from which it could presumably fall; the presence of traces on the corpse, especially uncharacteristic of the surface on which the corpse is located; the presence of damage on the corpse uncharacteristic of a fall on the surface on which the corpse is located; traces of biological origin on an object from which the deceased could have fallen, etc.
For gunshot injuries: it is necessary to study in detail the nature of the damage to the body and clothing; the presence of marks on clothing and on foreign objects in the area of damage; the relative position of damage and traces of biological origin on objects at the scene of the incident; upon detection of an alleged instrument of injury, determine the presence of traces of biological origin on it, etc.
For mechanical asphyxia: you should pay attention to the presence of puffiness of the face; the presence of marks on the neck, face and chest, the presence of pinpoint hemorrhages in the membranes of the eyes; identify objects at the scene that could have been used to compress the neck or other parts of the body; establish the correspondence or inconsistency of the strangulation groove and the object used to compress the neck; location of cadaveric spots; presence and location of traces of biological origin, etc.
If drowning in water: identify the presence of objects that can hold the corpse on the water or objects that weigh down the corpse; the condition of the clothing and the presence of marks on it; presence and location of damage; location and severity of skin maceration; the presence of foam at the openings of the mouth and nose and some other signs.
In case of poisoning: conduct a thorough search for traces of damage from exposure to poison on the skin and clothing; look for marks on clothes and surrounding objects; determine the presence of vomit; identify empty containers that could contain poison; describe the condition of corpse stains, the presence of odors in the room, etc.
When exposed to low temperatures: describe the pose of the corpse; the condition of the surface on which the corpse is located; condition of the corpse's skin; nature of clothing; the presence of ice floes at the openings of the nose and mouth, near the eyes and some other features.
When exposed to high temperature: examine the condition of clothing, signs of burning and scorching; fix the pose of the corpse; localization, degree and extent of burns; the presence of unsmoked folds at the corners of the eyes; the presence of soot in the mouth and nose and other features inherent in various options for exposure to elevated temperature.
In case of electric shock: describe burns, melting and other damage to clothing; figures of lightning when struck by atmospheric electricity; presence of damage to objects surrounding the corpse; the presence of electrical marks on the skin; the presence of sections of electrical conductors that are open to parts of the human body and other signs.
When corpses of newborns are discovered: examine the means of packaging the child’s body, the nature of clothing, if any; presence of mechanical damage; umbilical cord condition; the presence of a child's seat and some other signs.
When examining the corpse of an unknown person: examine in detail and describe the clothes and objects found with the corpse; describe appearance, while following the rules developed for such cases; describe in detail the individual characteristics found on the corpse; photograph the corpse according to the rules of signal photography; if possible, fingerprint the corpse; carry out other actions aimed at collecting search and identification information.
If parts of a dismembered corpse are found: carefully describe all items used to package body parts; describe clothes; record the structural features of body parts; study and describe the nature of the damage, including the surfaces of separation; if possible, describe the appearance and fingerprint, carry out other necessary actions.
If you suspect a criminal abortion: describe the presence, location and size of traces of biological origin in combination with other traces; the presence of items that could be used to perform an abortion; signs of pregnancy; condition of the external genitalia; search for the fetus, its parts and placenta, and perform other actions.
In case of sudden death: determine the presence or absence of traces, including traces of biological origin, on furnishings; availability of medical documentation; establish the presence of injuries on the body and clothing, as well as other material and documentary evidence of sudden death.
In case of reasonable suspicion of death from a dangerous infectious disease (plague, smallpox, cholera, etc.): immediately report your suspicions to the investigator and take measures together with him to inform the heads of the nearest health authorities; close access to the place where the corpse was found; persons participating in the inspection should remain in place until the arrival of specialists from the anti-epidemic team and then follow the instructions of the senior officer of the arriving anti-epidemic service team.
Summing up and documenting the results of the inspection of the scene of the incident is an important stage in the work at the scene of the incident. At this stage, the investigator and other participants in the inspection analyze the collected data and evaluate how fully they managed to solve the assigned tasks. As a result of this analysis, omissions can be identified and corrected by re-examining key objects at the scene. In most cases, it is advisable to conduct a second cursory inspection of the scene. Taking into account the experience of an already completed inspection, you can discover previously unnoticed important details or take a fresh look at previously inspected areas of the scene.
Then the final version of the protocol is drawn up. The inspection report of the scene of the incident must be drawn up in at least two copies. The second copy (copy) must be sent to the forensic morgue along with the corpse.
The corpse from the place of its discovery must be sent to the morgue. In order to ensure the safety of the corpse before it is examined in the morgue, the investigator, with the participation of employees of territorial internal authorities, takes the necessary measures to pack it (it is advisable to use special technical means for this) and provide special transport. The use of passing transport is highly undesirable.
If a criminal case has not yet been initiated before the corpse is sent to the morgue, then the corpse is sent to the morgue with an accompanying document, from which it should be clear: where, by whom and for what purpose the corpse is sent. A copy (second copy) of the inspection report of the place where it was found, as well as all things found with the corpse and personal documents, must be sent with the corpse.
The equipment necessary for a forensic specialist to examine a corpse at the place of its discovery must be provided by health authorities.
Exhumation of corpses - removal of corpses from the ground - is carried out in cases where a human corpse was buried without its forensic medical examination, as well as in cases where the initial forensic medical examination of the corpse was carried out incompletely or new serious circumstances arose that require verification through research already buried corpse.
Exhumation is carried out only by order of the investigator.
When carrying out exhumation, a number of points must be taken into account:
It should be remembered that exhumation is an organizationally and technically very complex event, and can also cause serious moral trauma to the loved ones of the deceased person, so it is not advisable to prescribe it without serious reasons. Before ordering exhumation, you should consult with forensic doctors regarding the possibilities of determining certain data on a modified corpse in relation to a specific case.
Based on the results of the exhumation, an investigative inspection protocol is drawn up in accordance with the requirements set out above.
Inspection of accident scenes- a very important and responsible investigative action. What was missed during the inspection of the crime scene and the corpse is most often lost irretrievably and cannot be obtained by carrying out other investigative and other actions.
The most qualified personnel from among investigators, operational workers, forensic specialists and forensic doctors should be involved in the inspection of the crime scene and the corpse.
Law enforcement agencies practice dividing corpses into "criminal" And "non-criminal". The corpses of murdered people are considered “criminal” when the presence of a murder is absolutely obvious; corpses in all other cases are called “non-criminal”.
44. Early cadaveric changes. Mechanisms of occurrence. Forensic significance
Cooling of the body, cadaveric spots, rigor mortis, drying of tissues belong to early cadaveric phenomena.
When a corpse is cooled, the body temperature usually remains at the same level during the first tens of minutes after death. Sometimes, under the influence of microbes, it can rise to more than 40 °C.
The cooling of the corpse is caused by the cessation of metabolism and heat production. After 45–60 minutes, body temperature decreases uniformly by 1 °C per hour. The speed of the postmortem temperature drop is influenced by the ambient temperature, the location of the corpse, the presence of clothing, wind strength, weight and volume of the body, cause of death, etc.
Cadaveric spots. After cessation of blood circulation, blood and other body fluids move in accordance with physical laws: under the influence of gravity, they gradually descend to the underlying sections.
Blood seeps outside the vessels and accumulates in the tissues, giving them and the skin a dirty purple color with a predominance of various shades, depending on many reasons, including the cause of death.
In case of carbon monoxide poisoning, cadaveric spots have a bright red color (blood hemoglobin turns into carboxyhemoglobin); in case of poisoning with cyanide compounds, they have a peculiar cherry color.
In the cold, the color of cadaveric spots is bright pink (due to the oxidation of hemoglobin by air oxygen penetrating through microcracks in the skin that form when body fluids freeze).
When hanging, if the corpse has not been removed from the noose for a long time, the cadaveric spots are predominantly located on the forearms, legs, and feet.
Stages of formation of cadaveric spots:
1) the stage of hypostasis continues for 12 hours after death. The liquid part of the blood is in the vessels, and when pressure is applied to the spots, the blood is squeezed out of the vessels, and after the pressure stops, it quickly fills them again;
2) the stage of stasis (diffusion) is observed after 12 hours from the moment of death and lasts up to 24 hours. Cadaveric spots turn pale, but do not disappear when pressed;
3) the imbibition stage develops on the second day after death. Cadaveric spots are well fixed, do not move, and do not turn pale when pressed, since the soft tissues are saturated with blood.
Forensic significance of cadaveric spots:
1) are the earliest sign of death;
2) reflect the position of the body and its possible changes after death - approximately allow one to determine the time of death;
3) the degree of severity reflects the speed of death;
4) the color of cadaveric spots in some poisonings serves as a diagnostic sign or it indicates the conditions in which the corpse was located;
5) make it possible to judge the nature of the objects on which the corpse was located.
From the book Motion sickness, its prevention and treatment author Mikhail Pavlovich EfremenkoMotion sickness. REASONS AND MECHANISMS OF ITS APPEARANCE Motion sickness is understood as a peculiar reaction of the human body to the action of inertial forces during movement, especially with a sharp change in the position in space of vehicles. Motion sickness manifests itself in
From the book Spinal Diseases. Complete guide author author unknownMECHANISMS OF APPEARANCE OF NEUROLOGICAL SYMPTOMATICS IN DISC HERNIA Action of direct mechanical factor. Even a slight displacement of the altered disc towards the spinal canal, combined with pressure on the posterior longitudinal ligament
From the book Normal Physiology: Lecture Notes author Svetlana Sergeevna Firsova From the book Normal Physiology author Marina Gennadievna Drangoy From the book Forensic Medical Examination: Problems and Solutions by E. S. Gordon4. Physico-chemical mechanisms of the emergence of the resting potential Membrane potential (or resting potential) is the potential difference between the outer and inner surfaces of the membrane in a state of relative physiological rest. The resting potential occurs at
From the book Forensic Medicine. Crib by V.V. Batalin5. Physico-chemical mechanisms of the occurrence of an action potential An action potential is a shift in the membrane potential that occurs in tissue under the action of a threshold and superthreshold stimulus, which is accompanied by recharging of the cell membrane. Upon action
From the book Complete Medical Diagnostics Guide by P. Vyatkin From the author's book9. Characteristics and forensic significance of abrasions and bruises An abrasion is a superficial mechanical damage to the epidermis of the skin or the epithelium of the mucous membranes. In the mechanism of their formation, the main role is played by the movement of an object along the surface of the body, and
From the author's book10. Characteristic features of wounds resulting from the action of blunt objects. Their forensic medical significance Mechanical damage to the integument of the body, penetrating deep into the dermis of the skin or into the subcutaneous (submucosal) tissue is called wounds. Injuries depending on the
From the author's book16. Mechanisms for the occurrence of damage when crossing with the wheel (wheels) of a vehicle As an independent type of automobile injury, crossing with a wheel (wheels) is rare, more often combined with an impact from a vehicle. Up to 90% of all crossings are made by trucks
From the author's book19. Railway injury. Mechanisms of damage. Issues resolved by forensic medical examination Railway injury refers to rail injury. Types of rail injuries have many similarities with types of car injuries. Mechanisms of formation
From the author's book23. Mechanisms of occurrence and characteristics of chopped wounds. Issues resolved by forensic medical examination Chopping tools are called axes, hoes, shovels, etc. The presence of a more or less sharp blade and a relatively large mass, as a rule, is their
From the author's book34. Drowning. Forensic significance. Signs of a long stay of a body in water Mechanical asphyxia, which develops when a person is immersed in liquid, is called drowning. By type of death, drowning is most often an accident; less often it is
From the author's book45. Late cadaveric changes. Causes of occurrence. Forensic significance Late cadaveric phenomena include fat wax, putrefaction, mummification, peat tanning, and preservation. The corpse may be subject to destruction or preservation as a result of the development of late
From the author's book53. Establishing the presence of blood on physical evidence. Forensic blood examination Determining the presence of blood. Blood samples are divided into two large groups: preliminary (indicative) and reliable (evidence). Preliminary samples
Changes in the color of the skin caused by the flow of blood into the underlying surfaces of the corpse (post-mortem redistribution of blood in a corpse).
Mechanism of formation of cadaveric spots
After the cessation of cardiac activity, blood pressure drops to zero, contraction of blood vessels in the arterial system continues for some time, which leads to overflow of capillaries and small veins; due to gravity, the blood drops, passively expanding the underlying venous vessels and begins to shine through the skin, forming cadaveric spots. They are usually purple with a blue tint and are formed by blood deprived of oxygen and containing reduced hemoglobin.
Location of cadaveric spots
The location of cadaveric spots depends on the position of the body of the corpse.
When the corpse is in a vertical position, cadaveric spots are located on the lower extremities, forearms, and hands. When the corpse is positioned on the back, they form on the posterolateral surfaces of the body, with the exception of areas subjected to compression. When the corpse is positioned on its stomach, they form on the front surface of the body (neck, chest, abdomen, lower extremities).
Degree of severity of cadaveric spots
The severity of cadaveric spots depends on the condition and amount of blood. With mechanical asphyxia, cadaveric spots are abundant, this is explained by the liquid state of the blood. With prolonged agony, the slow formation of cadaveric spots, as red and white convolutions are formed. With heavy blood loss, cadaveric spots are weakly expressed and slowly form.
Color of cadaveric spots
The color of cadaveric spots has important diagnostic value. In case of carbon monoxide poisoning, cadaveric spots are bright red due to the formation of carboxyoglobin. In case of poisoning with methemoglobin-forming poisons (nitrobenzene, berthollet salt, naphthalene, etc.), cadaveric spots acquire a grayish-brown color.
In case of death from hypothermia and drowning in water, cadaveric spots with a pinkish tint, as the epidermis loosens and oxygen penetrates into the blood forming oxyhemoglobin.
Stages of corpse spots
When examining cadaveric spots, the forensic expert, in addition to describing the nature, location and color of the cadaveric spots, must establish what stage they are in. To do this, pressure is applied to the cadaveric spot with the palmar surface of the nail phalanx of the index finger in those areas of the body where bone tissue is located under the skin (lumbar region, sternum). The pressure can be produced with a special dynamometer; the pressure force should be 2 kg per 1 square meter. see, pressure duration 3 seconds. The time of restoration of the color of the cadaveric spot is recorded with a stopwatch.
There is a certain pattern in the formation of cadaveric spots, where three stages of development of cadaveric spots are distinguished: hypostasis (cadaveric deposition), stasis (stop, diffusion) andimbibition (impregnation).
First stage- hypostasis begins immediately after cardiac arrest, and the earliest appearance of cadaveric spots is already after 30 minutes, if the death was not from blood loss and the blood in the corpse is liquid. The duration of the stage is from 8 to 16 hours. Typically, cadaveric spots appear 2 hours after death. Blood, almost unchanged in its properties, is located in the vessels of the underlying parts of the body under the influence of gravity. When you press on the cadaveric spot at this stage, it disappears, the blood is forced out of the vessels and restores its color. On the surface of the cut in the area of cadaveric spots, dilated venous vessels are visible, from which dark red, liquid blood flows.
If the position of the corpse is changed before 12 o'clock, then the cadaveric spots appear again on the underlying parts of the body and disappear on the overlying ones.
Second stage- stasis (diffusion). The duration of the stage is from 8-12 hours to 24-36 hours. In this period lymph and intercellular fluid gradually penetrate through the walls of blood vessels into them, gradually diluting the liquid part of the blood (plasma), promoting hemolysis (disintegration) of erythrocytes (red blood cells). Blood also penetrates the wall of blood vessels and permeates the surrounding tissue. Cadaveric spots at this stage do not disappear when pressed, but turn pale and slowly restore their original color. If the position of the corpse is changed 14-16 hours after death, then less intense cadaveric spots will still appear in the underlying sections, but will not disappear where they formed earlier. The second stage may occur earlier than 8 hours with blood loss or later than 16 hours with mechanical asphyxia. A reddish watery liquid flows from the cut surface in the area of the cadaveric spots, and drops of blood slowly flow from the cut vessels.
The third stage is imbibition (impregnation). It begins to develop 24-36 hours after death by the end of the first day. A fluid consisting of lymph, intercellular fluid, plasma, and hemolysis products permeate soft tissues and skin. Cadaveric spots at this stage do not turn pale or disappear when pressed, but retain their original color and do not move when the position of the corpse changes. On the cut tissue in the area of the cadaveric spot, a pinkish liquid flows from its surface, no blood is released from the cut vessels.
In the internal organs, simultaneously with the appearance of cadaveric spots in the skin of the corpse, a similar picture occurs in the underlying parts of the internal organs (cadaveric hypostases), blood accumulates in the internal organs, giving them a reddish-bluish appearance.

Representatives of these zodiac signs do not always become close people, but they are pleasant and interesting to each other. Unites...

Compatibility between a Rooster man and a Pig woman is based on mutual understanding between the partners. They have different personalities and...

According to many experts, the Unified State Exam 2016 will be the last in the history of modern Russian education. Next...
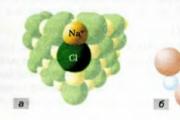
several basic concepts and formulas. All substances have different mass, density and volume. A piece of metal of one element...

If we’re going to talk about gender equality, then it’s with someone like an Aries woman. This emancipated lady is a shining example...

The meaning of life is related to the question “What to live for”, and not to the question of how to maintain life. A person's attitude is...

A mushroom is a living organism that forms a separate kingdom of the same name. For a long time they were classified as a kingdom...

For lovers of “quiet” hunting, mushroom season begins in early summer and lasts until late autumn. And rarely do they...

Aleshnikova, V.I. Use of professional consultants. - M.: Infra-M, 1999. - 240 p. 2. Beich, E....

Orange juice. The symbolic meaning of orange juice in dream books is pleasure and temptation. Enough...
We most often overcome all kinds of difficulties encountered along the path of life. Of course, for this we...

This year your patron Neptune will be in your constellation and this is a good sign, because you will...

1993 who? 1993 is the year of which animal? — According to the Chinese horoscope, 1873, 1933, 1993 belonged to the years of the Black...

Wave-particle duality of light means that light simultaneously has the properties of continuous...

Compatibility between a Rooster man and a Pig woman is based on mutual understanding between the partners. They have different personalities and...

According to many experts, the Unified State Exam 2016 will be the last in the history of modern Russian education. IN...