Philosophical vision of the problem
The meaning of life is related to the question “What to live for”, and not to the question of how to maintain life. A person's attitude is...
Diphtheria- acute anthroponotic bacterial infection with general toxic effects and fibrinous inflammation at the site of the pathogen's entrance gate.
The disease has been known since ancient times; Hippocrates, Homer, and Galen mention it in their works. Over the centuries, the name of the disease has changed several times: “fatal pharyngeal ulcer”, “Syrian disease”, “hangman’s noose”, “malignant tonsillitis”, “croup”. In the 19th century, P. Bretonneau, and later his student A. Trousseau, presented a classic description of the disease, identifying it as an independent nosological form called “diphtheria”, and then “diphtheria” (Greek diphthera - film, membrane).
E. Klebs (1883) discovered the pathogen in films from the oropharynx; a year later F. Loeffler isolated it in pure culture. A few years later, a specific diphtheria toxin was isolated (E. Roux and A. Yersin, 1888), an antitoxin was discovered in the patient’s blood, and an antitoxic anti-diphtheria serum was obtained (E. Roux, E. Bering, Sh. Kitazato, Y.Yu. Bardakh, 1892 -1894). Its use has reduced the mortality rate from diphtheria by 5-10 times. G. Ramon (1923) developed an anti-diphtheria toxoid. As a result of immunoprophylaxis, the incidence of diphtheria has sharply decreased; in many countries it has even been eliminated.
In Ukraine, since the late 70s and especially in the 90s of the 20th century, against the background of a decrease in collective antitoxic immunity, the incidence of diphtheria has increased, primarily in the adult population. This situation was caused by defects in vaccination and revaccination, the change of biovars of the pathogen to more virulent ones and the deterioration of the socio-economic living conditions of the population.
The causative agent of diphtheria- gram-positive, non-motile rod-shaped bacterium Corynebacterium diphtheriae. The bacteria have club-shaped thickenings at the ends (Greek sogune - club). When dividing, cells diverge at an angle to each other, which determines their characteristic arrangement in the form of outstretched fingers, hieroglyphs, Latin letters V, Y, L, parquet, etc. Bacteria form volutin, the grains of which are located at the poles of the cell and are revealed by staining. According to Neisser, bacteria are colored brownish-yellow with blue thickened ends. There are two main biovars of the pathogen (gravis and mitts), as well as a number of intermediate ones (intermedius, minimus, etc.). Bacteria are fastidious and grow on serum and blood media. The most widespread are media with tellurite (for example, Clauberg II medium), since the pathogen is resistant to high concentrations of potassium or sodium tellurite, which inhibits the growth of contaminating microflora. The main factor of pathogenicity is diphtheria exotoxin, classified as a potent bacterial poison. It is second only to botulinum and tetanus toxins. Only lysogenic strains of the pathogen infected with a bacteriophage carrying the tox gene, encoding the structure of the toxin, exhibit the ability to form toxins. Nontoxigenic strains of the pathogen are not capable of causing disease. Adhesiveness, i.e. the ability to attach to the mucous membranes of the body and multiply determines the virulence of the strain. The pathogen persists for a long time in the external environment (on the surface of objects and in dust - up to 2 months). Under the influence of a 10% solution of hydrogen peroxide it dies after 3 minutes, when treated with a 1% solution of sublimate, a 5% solution of phenol, 50-60° ethyl alcohol - after 1 minute. Resistant to low temperatures; when heated to 60 ° C, it dies within 10 minutes. Ultraviolet rays, chlorine-containing preparations, Lysol and other disinfectants also have an inactivating effect.
Reservoir and source of infection- a sick person or a carrier of toxigenic strains. The greatest role in the spread of infection belongs to patients with oropharyngeal diphtheria, especially those with erased and atypical forms of the disease. Convalescents release the pathogen for 15-20 days (sometimes up to 3 months). Bacteria carriers that secrete the pathogen from the nasopharynx pose a great danger to others. In different groups, the frequency of long-term carriage varies from 13 to 29%. The continuity of the epidemic process ensures long-term carriage even without registered morbidity.
Transmission mechanism- aerosol, transmission route - airborne droplets. Sometimes transmission factors can be contaminated hands and environmental objects (household items, toys, dishes, linen, etc.). Diphtheria of the skin, eyes and genitals occurs when the pathogen is transmitted through contaminated hands. Foodborne outbreaks of diphtheria are also known, caused by the multiplication of the pathogen in milk, confectionery creams, etc.
Natural sensitivity of people high and determined by antitoxic immunity. The blood content of 0.03 AE/ml of specific antibodies provides protection against the disease, but does not prevent the formation of carriage of pathogenic pathogens. Diphtheria antitoxic antibodies, transmitted transplacentally, protect newborns from the disease during the first six months of life. People who have had diphtheria or are properly vaccinated develop antitoxic immunity, its level is a reliable criterion of protection against this infection.
Basic epidemiological signs. Diphtheria, as a disease that depends on the vaccination of the population, according to WHO experts, can be successfully controlled. In Europe, extensive immunization programs began in the 1940s, and the incidence of diphtheria quickly decreased to isolated cases in many countries. A significant decrease in the immune layer always accompanies an increase in the incidence of diphtheria. This happened in Ukraine in the early 90s, when, against the backdrop of a sharp decline in collective immunity, an unprecedented increase in morbidity was noted, primarily among adults. Following the increase in morbidity among adults, children who did not have antitoxic immunity were also involved in the epidemic process, often as a result of unjustified refusals from vaccinations. Population migration in recent years has also contributed to the widespread spread of the pathogen. Periodic (over long-term dynamics) and autumn-winter (intra-annual) increases in incidence are also observed due to defects in vaccine prevention. Under these conditions, the incidence may “shift” from childhood to older age, predominantly affecting people in endangered professions (transport, trade, service sector workers, medical workers, teachers, etc.). A sharp deterioration in the epidemiological situation is accompanied by a more severe course of the disease and an increase in mortality. The rise in the incidence of diphtheria coincided with an increase in the breadth of circulation of the gravis and intermedius biovars. Among the cases, adults still predominate. Among vaccinated people, diphtheria occurs easily and is not accompanied by complications. The introduction of infection into a somatic hospital is possible during the hospitalization of a patient with an erased or atypical form of diphtheria, as well as a carrier of a toxigenic pathogen.
The main entrance gates of infection- mucous membranes of the oropharynx, less often - the nose and larynx, even less often - the conjunctiva, ears, genitals, skin. The pathogen multiplies in the area of the entrance gate. Toxigenic strains of bacteria secrete exotoxin and enzymes, provoking the formation of a focus of inflammation. The local effect of diphtheria toxin is expressed in coagulative necrosis of the epithelium, the development of vascular hyperemia and blood stasis in the capillaries, and increased permeability of the vascular walls. Exudate containing fibrinogen, leukocytes, macrophages and often erythrocytes extends beyond the vascular bed. On the surface of the mucous membrane, as a result of contact with thromboplastin of necrotic tissue, fibrinogen is converted into fibrin. The fibrin film is firmly fixed on the multilayer epithelium of the pharynx and pharynx, but is easily removed from the mucous membrane covered with single-layer epithelium in the larynx, trachea and bronchi. However, with a mild course of the disease, inflammatory changes can be limited only to a simple catarrhal process without the formation of fibrinous plaques.
The pathogen's neuraminidase significantly potentiates the action of the exotoxin. Its main part is histotoxin, which blocks protein synthesis in cells and inactivates the transferase enzyme responsible for the formation of polypeptide bonds.
Diphtheria exotoxin spreads through the lymphatic and blood vessels, causing the development of intoxication, regional lymphadenitis and edema of surrounding tissues. In severe cases, swelling of the uvula, palatine arches and tonsils sharply narrows the entrance to the pharynx, and swelling of the cervical tissue develops, the degree of which corresponds to the severity of the disease.
Toxinemia leads to the development of microcirculatory disorders and inflammatory and degenerative processes in various organs and systems - the cardiovascular and nervous systems, kidneys, adrenal glands. The binding of the toxin to specific cell receptors occurs in two phases - reversible and irreversible.
- In the reversible phase, cells retain their viability, and the toxin can be neutralized by antitoxic antibodies.
- In the irreversible phase, antibodies can no longer neutralize the toxin and do not interfere with the implementation of its cytopathogenic activity.
As a result, general toxic reactions and sensitization phenomena develop. Autoimmune mechanisms may play a certain role in the pathogenesis of late complications of the nervous system.
Antitoxic immunity that develops after diphtheria does not always protect against the possibility of recurrent disease. Antitoxic antibodies have a protective effect in titers of at least 1:40.
Incubation period lasts from 2 to 10 days. The clinical classification of diphtheria divides the disease into the following forms and course options.
Oropharyngeal diphtheria accounts for 90-95% of all cases of the disease in children and adults; in 70-75% of patients it occurs in a localized form. The disease begins acutely, elevated body temperature from subfebrile to high persists for 2-3 days. Moderate intoxication: headache, malaise, loss of appetite, pale skin, tachycardia. With a decrease in body temperature, local manifestations in the area of the entrance gate persist and may even increase. The intensity of pain in the throat when swallowing corresponds to the nature of the changes in the oropharynx, where mild congestive diffuse hyperemia, moderate swelling of the tonsils, soft palate and arches are noted. The plaques are localized only on the tonsils and do not go beyond their boundaries; they are located in separate islands or in the form of a film (islet or filmy options). Fibrinous deposits in the first hours of the disease look like a jelly-like mass, then like a thin cobweb-like film, but already on the 2nd day of the disease they become dense, smooth, grayish in color with a pearlescent sheen, are difficult to remove, and when they are removed with a spatula, the mucous membrane bleeds. The next day, a new one appears in place of the removed film. The removed fibrinous film, placed in water, does not disintegrate and sinks. In the localized form of diphtheria, typical fibrinous plaques are observed in no more than 1/3 of adult patients; in other cases, as well as at a later stage (3-5th day of illness), the plaques are loosened and removed easily; there is no bleeding of the mucous membrane when they are removed. expressed. Regional and submandibular lymph nodes are moderately enlarged and sensitive to palpation. The process in the tonsils and the reaction of regional lymph nodes can be asymmetrical or one-sided.
Catarrhal variant localized diphtheria of the oropharynx is rarely recorded; it is accompanied by minimal general and local symptoms. With normal or short-term subfebrile body temperature and mild manifestations of intoxication, unpleasant sensations in the throat when swallowing, slight hyperemia of the mucous membrane of the oropharynx, and swelling of the tonsils occur. The diagnosis of diphtheria in such cases can be made only taking into account the medical history, the epidemic situation and the results of laboratory examination.
The course of localized diphtheria of the oropharynx is usually benign. After normalization of body temperature, the sore throat decreases and then disappears, while plaque on the tonsils can persist for 6-8 days. However, if left untreated, the localized form of oropharyngeal diphtheria can progress and develop into other, more severe forms.
A common form of oropharyngeal diphtheria. They are relatively rare (3-11%). It differs from the localized form by the spread of plaque beyond the tonsils to any part of the mucous membrane of the oropharynx. Symptoms of general intoxication, swelling of the tonsils, tenderness of the submandibular lymph nodes are usually more pronounced than in the localized form. There is no swelling of the subcutaneous tissue of the neck.
Subtoxic form of oropharyngeal diphtheria. Phenomena of intoxication, severe pain when swallowing and sometimes in the neck area are noted. The tonsils are purplish-cyanotic in color with plaque that is localized or slightly extending to the palatine arches and uvula. Swelling of the tonsils, arches, uvula and soft palate is moderate. Enlargement, tenderness and density of regional lymph nodes are noted. A distinctive feature of this form is local swelling of the subcutaneous tissue above the regional lymph nodes, often one-sided.
Toxic form of oropharyngeal diphtheria. Currently, it occurs quite often (about 20% of the total number of patients), especially in adults. It can develop from an untreated localized or widespread form, but in most cases it occurs immediately and progresses rapidly. Body temperature is usually high (39-41 °C) from the first hours of the disease. Headache, weakness, severe pain in the throat, sometimes in the neck and abdomen are noted. Vomiting, painful trismus of the masticatory muscles, euphoria, agitation, delirium, and delirium may occur. The skin is pale (with toxic diphtheria stage III, facial hyperemia is possible). Diffuse hyperemia and pronounced edema of the mucous membrane of the oropharynx, which completely covers the lumen of the pharynx in toxic diphtheria of II and III degrees, precede the appearance of fibrinous deposits. The resulting plaque quickly spreads to all parts of the oropharynx. Subsequently, fibrin films become thicker and rougher, lasting up to 2 weeks or more. The process is often one-sided. Regional lymph nodes enlarge early and significantly, become dense, painful, and periadenitis develops.
Local manifestations of toxic diphtheria of the oropharynx differ from all other forms of the disease by the presence of painless doughy swelling of the subcutaneous tissue of the neck, reaching its middle in toxic diphtheria of the I degree, of the collarbone - in the II degree. In grade III, the swelling descends below the collarbone, can spread to the face, back of the neck, back and progresses rapidly.
A general toxic syndrome is expressed, cyanosis of the lips, tachycardia, and decreased blood pressure are noted. As body temperature decreases, symptoms remain severe. A specific sickly putrid odor emanates from the patients’ mouths, and their voice takes on a nasal tone.
Toxic diphtheria of the oropharynx is often combined with lesions of the larynx and nose. Such combined forms are characterized by a severe course and are difficult to treat.
Hypertoxic form- the most severe manifestation of diphtheria. It develops more often in patients with an unfavorable premorbid background (alcoholism, diabetes mellitus, chronic hepatitis, etc.). Body temperature with chills quickly increases to high numbers, intoxication is pronounced (weakness, headache, vomiting, dizziness, signs of encephalopathy). Progressive hemodynamic disorders are noted - tachycardia, weak pulse, decreased blood pressure, pallor, acrocyanosis. Skin hemorrhages, organ bleeding, and fibrinous plaques are soaked in blood, which reflects the development of disseminated intravascular coagulation syndrome. The clinical picture is dominated by signs of rapidly developing infectious-toxic shock, which can cause the death of the patient already on the 1st-2nd day of the disease.
There are localized (diphtheria of the larynx) and widespread (with simultaneous damage to the larynx, trachea and even bronchi) forms. The common form is often combined with diphtheria of the oropharynx and nose. Recently, this form of diphtheria is quite often found in adult patients. Clinically, croup manifests itself in the form of three sequentially developing stages - dysphonic, stenotic and asphyxic - with moderate symptoms of intoxication.
Due to the anatomical features of the larynx in adults, the development of diphtheria croup takes longer than in children; retraction of the compliant areas of the chest may be absent. In some cases, the only signs of this form of the disease are hoarseness and a feeling of shortness of breath. At the same time, attention is drawn to pallor of the skin, weakened breathing, tachycardia, and a decrease in oxygen tension when studying the acid-base state. Unconditional assistance in making a diagnosis is provided by laryngoscopic (in some cases, bronchoscopic) examination, which reveals hyperemia and edema of the larynx, films in the vocal cords, damage to the trachea and bronchi.
Characterized by minor intoxication, difficulty in nasal breathing, serous-purulent or sanguineous discharge (catarrhal variant). The nasal mucosa is hyperemic, edematous, with erosions, ulcers or fibrinous deposits in the form of easily removable “shreds” (membranous version). The skin around the nose becomes irritated, weepy, and crusty. Nasal diphtheria usually develops in combination with damage to the oropharynx and (or) larynx, and sometimes the eyes.
It can occur in catarrhal, membranous and toxic forms.
With the catarrhal variant, inflammation of the conjunctiva (usually unilateral) with light discharge is noted. Body temperature is normal or subfebrile. There are no symptoms of intoxication or regional lymphadenitis.
In the membranous variant, against the background of subfebrile body temperature and mild general toxic phenomena, a fibrin film is formed on the hyperemic conjunctiva, swelling of the eyelids increases, and serous-purulent discharge appears. The process is initially one-sided, but after a few days it can spread to the other eye.
Toxic diphtheria of the eyes has an acute onset and is characterized by the rapid development of symptoms of intoxication, swelling of the eyelids, copious purulent secretions, irritation and weeping of the skin around the eye. The swelling spreads, affecting various areas of the subcutaneous tissue of the face. Membranous conjunctivitis is often accompanied by lesions of other parts of the eye, including panophthalmia, as well as regional lymphadenitis.
These conditions are rare; they usually develop in combination with diphtheria of the pharynx or nose. The common features of these forms are edema, hyperemia, infiltration, fibrinous plaque in the affected area, regional lymphadenitis.
With diphtheria of the genital organs in men, the process is localized in the area of the foreskin. In women, it can become widespread and involve the labia, vagina, perineum and anus, accompanied by serous-bloody vaginal discharge, difficult and painful urination.
Diphtheria of the skin develops in the area of wounds, diaper rash, eczema, fungal infections with skin cracks, where a dirty gray coating with serous-purulent discharge is formed. General toxic effects are insignificant, but the local process regresses slowly (up to 1 month or more).
The development of these forms is facilitated by trauma to areas of the mucous membranes or skin, and the introduction of pathogens by hand.
In persons who have had diphtheria or have never had it, asymptomatic carriage can be observed, the duration of which varies significantly. The formation of carriage is facilitated by concomitant chronic diseases of the nasopharynx. Antitoxic immunity does not prevent the development of carriage.
Pathogenetically caused complications of diphtheria include infectious-toxic shock, myocarditis, mono- and polyneuritis, including lesions of the cranial and peripheral nerves, polyradiculoneuropathy, adrenal lesions, and toxic nephrosis. The frequency of their development in the localized form of oropharyngeal diphtheria is 5-20%, with more severe forms it increases significantly: with subtoxic diphtheria - up to 50% of cases, with varying degrees of toxic diphtheria - from 70 to 100%. The time for the development of complications, counting from the onset of the disease, depends primarily on the clinical form of diphtheria and the severity of the process. Severe myocarditis, which is the most common complication of toxic diphtheria, occurs early - at the end of the first or beginning of the 2nd week of the disease. Moderate and mild myocarditis is detected later, at 2-3 weeks. Toxic nephrosis, as a common complication of only toxic diphtheria, is detected by the results of urine tests already in the acute period of the disease. Manifestations of neuritis and polyradiculoneuropathy can occur both against the background of clinical manifestations of the disease and 2-3 months after recovery.
Localized and widespread diphtheria of the oropharynx is differentiated from tonsillitis of various etiologies (coccal, Simanovsky-Vincent-Plaut's tonsillitis, syphilitic, tularemia, etc.), infectious mononucleosis, Behçet's syndrome, stomatitis. It is distinguished by moderate intoxication, pale skin, mild hyperemia of the oropharynx, and slow regression of the manifestations of sore throat with a decrease in body temperature. In the filmy variant, the fibrinous nature of the deposits greatly facilitates diagnosis. The most difficult for differential diagnosis is the island variant of oropharyngeal diphtheria, which is often clinically indistinguishable from tonsillitis of coccal etiology.
When diagnosing toxic diphtheria of the oropharynx, it is necessary to carry out differential diagnosis with peritonsillar abscess, necrotizing tonsillitis due to blood diseases, candidiasis, chemical and thermal burns of the oral cavity. Toxic diphtheria of the oropharynx is characterized by rapidly spreading fibrinous deposits, swelling of the mucous membrane of the oropharynx and subcutaneous tissue of the neck, pronounced and rapidly progressing manifestations of intoxication.
Diphtheria croup is differentiated from false croup in measles, ARVI and other diseases. Croup is often combined with diphtheria of the oropharynx or nose, and clinically manifests itself in the form of three successively developing stages: dysphonic, stenotic and asphyxic with moderate symptoms of intoxication.
In the hemogram, with a localized form of diphtheria, moderate, and with toxic forms, high leukocytosis, neutrophilia with a shift of the leukocyte formula to the left, an increase in ESR, and progressive thrombocytopenia are noted.
The basis of laboratory diagnostics is bacteriological studies: isolation of the pathogen from the source of inflammation, determination of its type and toxigenicity. The material is taken with sterile cotton swabs, dry or moistened (before sterilization!) with a 5% glycerin solution. During storage and transportation, tampons are protected from cooling and drying out. The material must be sown no later than 2-4 hours after collection. In patients with tonsillitis who have been in contact with patients with diphtheria, as well as in persons with typical clinical manifestations of diphtheria, the diagnosis is made even if the result of a bacteriological examination is negative.
Of auxiliary importance is the determination of titers of antitoxic antibodies in paired sera when staging RNGA. Toxin formation is detected using RNGA with an antibody erythrocyte diagnosticum. It has been proposed to use PCR to detect diphtheria toxin.
All patients with diphtheria or suspected of having it are subject to hospitalization. The length of stay of patients in the hospital and the duration of bed rest depend on the form and severity of the disease. The main treatment for diphtheria is considered administration of antitoxic diphtheria serum. It neutralizes the toxin circulating in the blood, therefore, has the greatest effect when used early. If a toxic form of diphtheria or diphtheria croup is suspected, serum is administered immediately; in other cases, waiting may be possible with constant monitoring of the patient in a hospital. In patients with a localized form of diphtheria, they try not to use serum after the 4th day of illness, which, according to modern data, significantly reduces the possibility of developing long-term complications of the disease. Positive results of a skin test (Chick test) are a contraindication to the administration of serum only in localized forms; in all other cases in this situation, the serum must be administered under the cover of antihistamines and glucocorticoids.
Anti-diphtheria serum can be administered either intramuscularly (more often) or intravenously. Repeated administration of serum is possible with ongoing intoxication. Currently, serum doses are being revised both upward and downward, depending on the form of diphtheria.
Conduct detoxification therapy crystalloid and colloid solutions intravenously (polyionic solutions, glucose-potassium mixture with the addition of insulin, rheopolyglucin, fresh frozen plasma). In severe cases, glucocorticoids (prednisolone at a dose of 2-5 mg/kg) are added to the injected solutions. At the same time, these drip infusions help correct hemodynamic disorders. Desensitizing drugs and vitamins (ascorbic acid, B vitamins, etc.) are used.
Toxic diphtheria of II and III degrees, hypertoxic form and severe combined forms of the disease are indications for plasmapheresis. New effective ways of detoxification are being developed, such as hemosorption, affinity sorption, and immunosorption.
For subtoxic and toxic forms it is recommended prescribing antibiotics, which have an etiotropic effect on the accompanying coccal flora: penicillin, erythromycin, as well as ampicillin, ampiox, tetracycline drugs and cephalosporins in average therapeutic doses.
For diphtheria of the larynx, frequent ventilation of the room, warm drinks, steam inhalations with chamomile, soda, eucalyptus, hydrocortisone (125 mg per inhalation) are necessary. Patients are prescribed aminophylline, saluretics, antihistamines, and if stenosis increases, intravenous prednisolone 2-5 mg/kg/day. In cases of hypoxia, humidified oxygen is used through a nasal catheter, and films are removed using an electric suction.
Indications for surgery- progression of signs of respiratory failure: tachypnea more than 40 per minute, cyanosis, tachycardia, restlessness, hypoxemia, hypercapnia, respiratory acidosis. In this case, with localized croup, tracheal intubation is performed, with widespread, descending croup and a combination of croup with severe forms of diphtheria - tracheostomy followed by mechanical ventilation.
If signs of infectious-toxic shock occur, the patient is transferred to the intensive care unit. Along with active therapy through intravenous infusions of solutions, the dose of prednisolone is increased to 5-20 mg/kg. In addition, dopamine (200-400 mg in 400 ml of 10% glucose solution intravenously at a rate of 5-8 ml/kg/min), trental (2 mg/kg intravenously in 50 ml of 10% glucose solution), trasylol or kontrikal (up to 2000-5000 units/kg/day intravenously), saluretics, isadrin.
To sanitize bacterial secretions, clindamycin 150 mg 4 times a day, benzylpenicillin-novocaine salt 600,000 units 2 times a day intramuscularly, as well as cephalothin and cephaleandol parenterally in medium therapeutic doses are used. Course duration is 7 days. It is advisable to simultaneously treat chronic pathology of the ENT organs.
Epidemiological surveillance involves collecting information on the basis of which appropriate preventive measures can be taken. It includes not only monitoring the incidence and vaccination coverage, but also studying the immunological structure of the population, monitoring the circulation of the pathogen among the population, its biological properties and antigenic structure. Of great importance are epidemiological analysis and assessment of the effectiveness of the measures taken, forecasting the intensity of the epidemic process of diphtheria in a specific territory.
Vaccine prevention remains the main way to control diphtheria. The immunization scheme for children provides for immunization with the DTP vaccine starting from the 3rd month of life (vaccinated 3 times with an interval of 30-40 days). Revaccination is carried out 9-12 months after completed vaccination. For revaccination at 6-7, 11-12 and 16-17 years old, ADS-M is used. In some cases, for example, when there are contraindications to the pertussis component of DPT, ADS-M is also used for vaccination. In the modern epidemiological situation, immunization of adults has acquired particular importance. Among adults, people from high-risk groups are vaccinated first:
For adult vaccinations, ADS-M is used in the form of routine immunization every 10 years until age 56 inclusive. Persons who have had diphtheria are also subject to vaccinations. The disease of any form of diphtheria in unvaccinated children and adolescents is regarded as the first vaccination, and in those who received one vaccination before the disease - as the second vaccination. Further vaccinations are carried out according to the current vaccination calendar. Children and adolescents who have been vaccinated against diphtheria (who have received complete vaccination, one or more revaccinations) and who have had a mild form of diphtheria without complications are not subject to additional vaccination after the disease. The next age-related revaccination is carried out in accordance with the intervals provided for by the current vaccination calendar.
Children and adolescents vaccinated against diphtheria (who have received completed vaccination, one or more revaccinations) and have suffered toxic forms of diphtheria should be vaccinated with the drug depending on age and health status - once in a dose of 0.5 ml, but not earlier than 6 months after an illness. Adults who have previously been vaccinated (received at least one vaccination) and have had a mild form of diphtheria are not subject to additional vaccination against diphtheria. If they suffer from a toxic form of diphtheria, they should be immunized against diphtheria, but not earlier than 6 months after the illness. Their revaccination should be carried out after 10 years. Persons with an unknown vaccination history are subject to serological testing for antitoxic antibodies. In the absence of a protective titer of antitoxins (more than 1:20), they are subject to vaccination.
The effectiveness of vaccination against diphtheria depends both on the quality of vaccine preparations and on the vaccination coverage of the population susceptible to this infection. The WHO Expanded Program on Immunization states that only 95% vaccination coverage guarantees vaccination effectiveness.
The spread of diphtheria is prevented through early identification, isolation and treatment of patients and carriers of toxigenic diphtheria bacilli. Of great preventive importance is the active identification of patients with diphtheria, which includes an annual scheduled examination of children and adolescents during the formation of organized teams. For the purpose of early detection of diphtheria, the local doctor (pediatrician, general practitioner) is obliged to actively monitor patients with tonsillitis with pathological deposits on the tonsils within 3 days from the initial treatment with a mandatory bacteriological examination for diphtheria during the first 24 hours.
Patients with diphtheria are subject to hospitalization, and if hospitalization is delayed, they are urgently administered 5000 IU of anti-diphtheria serum. Patients with severe forms of sore throat, patients from children's institutions with permanent stay of children (children's homes, orphanages, etc.), dormitories, living in unfavorable living conditions, persons belonging to the risk groups of diphtheria (medical workers, workers of preschool institutions, health and educational institutions, trade, catering, and transport workers) must be hospitalized for provisional purposes. Patients with sore throat with plaque or croup from the source of diphtheria are also subject to hospitalization.
Discharge from the hospital is allowed after clinical recovery and receipt of a 2-fold negative result of a bacteriological examination of mucus from the throat and nose for the presence of the causative agent of diphtheria, carried out at 2-day intervals, and no earlier than 3 days after the cessation of antibiotic therapy. A carrier of toxigenic diphtheria bacilli is discharged after receiving a 2-fold negative result of a bacteriological examination. After discharge from the hospital, patients and carriers of toxigenic diphtheria bacilli are immediately allowed to work, study and to children's institutions with permanent residence for children without additional bacteriological examination. If a carrier of toxigenic diphtheria bacilli continues to excrete the pathogen, despite two courses of sanitation with antibiotics, he is allowed to work, study, and preschool institutions. In these groups, all persons who have not previously been vaccinated against diphtheria must receive vaccination according to the current immunization schedule. Only people vaccinated against diphtheria are accepted into this team again.
Convalescents of diphtheria and carriers of diphtheria bacilli are subject to dispensary observation for 3 months after discharge from the hospital. Clinical examination is carried out by a local therapist and a doctor at the office of infectious diseases in the clinic at the place of residence.
The doctor who made the diagnosis immediately sends an emergency notification to the Center for Sanitary and Epidemiological Surveillance. When isolating the source of infection, wet cleaning is carried out using disinfectants, and final disinfection of toys, bedding, and linen is carried out. Bacteriological examination of persons who interacted with the patient is carried out once. Only persons who have had direct contact with a patient or a carrier of toxigenic strains of C. dyphtheriae are subject to serological examination in foci of diphtheria infection, in the absence of documentary evidence of the fact that they have been vaccinated against diphtheria. Medical observation of them (including examination by an otolaryngologist) continues for 7 days. Identified patients and carriers of toxigenic diphtheria bacilli are hospitalized. Carriers of non-toxigenic strains are not subject to treatment with antimicrobial drugs; they are advised to consult an otolaryngologist, identify and treat pathological processes in the nasopharynx. In the source of infection, persons who have not been vaccinated against diphtheria should be vaccinated, as well as children and adolescents who are due for their next vaccination or revaccination. Among adults, vaccination is subject to persons who, according to medical documentation, have been 10 years or more since their last vaccination, as well as persons with low antibody titers (less than 1:20), which are detected in the RPGA.
Is something bothering you? Do you want to know more detailed information about Diphtheria, its causes, symptoms, methods of treatment and prevention, the course of the disease and diet after it? Or do you need an inspection? You can make an appointment with a doctor– clinic Eurolab always at your service! The best doctors will examine you, study external signs and help you identify the disease by symptoms, advise you and provide the necessary assistance and make a diagnosis. you also can call a doctor at home. Clinic Eurolab open for you around the clock.
How to contact the clinic:
Phone number of our clinic in Kyiv: (+38 044) 206-20-00 (multi-channel). The clinic secretary will select a convenient day and time for you to visit the doctor. Our coordinates and directions are indicated. Look in more detail about all the clinic’s services on it.
(+38 044) 206-20-00
If you have previously performed any research, Be sure to take their results to a doctor for consultation. If the studies have not been performed, we will do everything necessary in our clinic or with our colleagues in other clinics.
You? It is necessary to take a very careful approach to your overall health. People don't pay enough attention symptoms of diseases and do not realize that these diseases can be life-threatening. There are many diseases that at first do not manifest themselves in our body, but in the end it turns out that, unfortunately, it is too late to treat them. Each disease has its own specific signs, characteristic external manifestations - the so-called symptoms of the disease. Identifying symptoms is the first step in diagnosing diseases in general. To do this, you just need to do it several times a year. be examined by a doctor, in order not only to prevent a terrible disease, but also to maintain a healthy spirit in the body and the organism as a whole.
If you want to ask a doctor a question, use the online consultation section, perhaps you will find answers to your questions there and read self care tips. If you are interested in reviews about clinics and doctors, try to find the information you need in the section. Also register on the medical portal Eurolab to keep abreast of the latest news and information updates on the site, which will be automatically sent to you by email.
What is diphtheria? We will discuss the causes, diagnosis and treatment methods in the article by Dr. P. A. Aleksandrov, an infectious disease specialist with 11 years of experience.
Diphtheria(from the Latin diftera - film; pre-revolutionary - “disease of crying mothers”, “disease of horror of mothers”) - an acute infectious disease caused by toxigenic strains of diphtheria bacillus, which toxically affect the circulatory system, nervous tissue and adrenal glands, and also cause fibrinous inflammation in the area entrance gates (places of infection). Clinically characterized by a syndrome of general infectious intoxication, maxillary lymphadenitis, tonsillitis, local inflammatory processes of a fibrinous nature.
Kingdom – Bacteria
genus – Corynebacterium
species – Corynebacterium diphteriae
These are gram-negative rods located at an angle V or W. At the ends there are club-shaped thickenings (from the Greek coryne - club) due to volutin granules. There is a property of metachromasia - staining not in the color of the dye (according to Neisser - dark blue, and bacterial cells - light brown).
Contains lipopolysaccharide, proteins and lipids. The cell wall contains a cord factor, which is responsible for adhesion (sticking) to cells. Colonies of mitis, intermedius, gravis are known. They remain viable in the external environment: under normal conditions they remain alive in the air for up to 15 days, in milk and water they live up to 20 days, on the surfaces of things - up to 6 months. They lose their properties and die when boiled for 1 minute, in 10% hydrogen peroxide - in 3 minutes. Sensitive to disinfectants and antibiotics (penicillins, aminopenicillins, cephalosporins). They love nutrient media containing sugar (McLeod's chocolate medium).
Identifies pathogenic products such as:
1) Exotoxin (synthesis of the toxin is determined by the tox+ gene, which is sometimes lost), including several components:
2) Neuraminidase;
3) Cystinase (allows you to distinguish diphtheria bacteria from other types of corynebacteria and diphtheroids).

Anthroponosis. The generator of the infection is a person suffering from various forms of diphtheria and a healthy carrier of toxigenic strains of diphtheria microbes. A possible source of infection for people is domestic animals (horses, cows, sheep), in which the pathogen can be localized on the mucous membranes, causing ulcers on the udder, mastitis.
The most dangerous in terms of the spread of infection are people with diphtheria of the nose, pharynx and larynx.
Transmission mechanisms: airborne droplets (aerosol), contact (through hands, objects), nutritional route (through milk).
A person is ill who does not have natural resistance (resistance) to the pathogen and does not have the required level of antitoxic immunity (0.03 - 0.09 IU/ml - conditionally protected, 0.1 and higher IU/ml - protected). After an illness, immunity lasts for about 10 years, then a recurrence of the disease is possible. The incidence of disease is affected by the coverage of the population with preventive vaccinations. Seasonality: autumn-winter. When carrying out a full course of immunization against diphtheria in childhood and regular revaccination (once every 10 years), a strong strong immunity is developed and maintained, protecting against the disease.
Despite the successes of modern healthcare, the mortality rate from diphtheria at the global level (mainly underdeveloped countries) remains within 10%.
The incubation period is from 2 to 10 days.
The course of the disease is subacute (i.e., the main syndrome appears 2-3 days from the onset of the disease), however, with the development of the disease at a young and mature age, as well as with concomitant pathologies of the immune system, it may change.
Diphtheria syndromes:
The onset of the disease is usually accompanied by a moderate rise in body temperature and general malaise, then the clinical picture diverges depending on the form of the disease.
Atypical form(characterized by short-term fever for two days, mild discomfort and painful sensation in the throat during swallowing, enlargement of the maxillary lymph nodes up to 1 cm, slightly sensitive to a light touch);

Typical shape(quite noticeable heaviness in the head, drowsiness, lethargy, weakness, pale skin, enlargement of the maxillary lymph nodes of 2 cm or more, pain when swallowing):
a) common(primarily widespread or developing from localized) - increased body temperature to febrile levels (38-39°C), noticeably expressed weakness, adynamia, pallor of the skin, dry mouth, sore throat when swallowing of moderate intensity, painful lymph nodes up to 3 cm ;
b) toxic(primarily toxic or originating from a common one) – characterized by severe headache, apathy, lethargy, pale skin, dry oral mucosa, possible abdominal pain in children, vomiting, temperature 39-41 ° C, painful sensations in the throat when swallowing , painful lymph nodes up to 4 cm, swelling of the subcutaneous fatty tissue around them, spreading in some cases to other parts of the body, difficulty in nasal breathing - nasal voice.
Degrees of swelling of subcutaneous fat tissue:
In severe toxic forms of diphtheria, due to edema, the neck visually becomes short and thick, the skin resembles a gelatinous consistency (the “Roman consuls” symptom).
The pallor of the skin is proportional to the degree of intoxication. Plaques on the tonsils are asymmetrical.
c) hypertoxic– acute onset, pronounced syndrome of general infectious intoxication, obvious changes in the site of the entrance gate, hyperthermia from 40°C; Acute cardiovascular failure and unstable blood pressure develop;
d) hemorrhagic– impregnation of fibrinous deposits with blood, bleeding from the nasal passages, petechiae on the skin and mucous membranes (red or purple spots formed when capillaries are damaged).
If, in the absence of adequate treatment, body temperature returns to normal, this cannot be clearly regarded as an improvement - it is often an extremely unfavorable sign.

There are rare diphtheria in vaccinated people (similar to atypical diphtheria) and diphtheria in combination with streptococcal infection (there are no fundamental differences).
Other forms of diphtheria infection:
Features of pharyngoscopy:
a) atypical (hyperemia and hypertrophy of the palatine tonsils);
b) typical (not pronounced redness with a bluish tint, filmy plaque, swelling of the tonsils. At the beginning of the disease it is white, then gray or yellow-gray; removed with pressure, tears - after removal it leaves a bleeding wound. The film is dense, insoluble and quickly sinks in water, protrudes above the tissue. It is characterized by low pain, since there is anesthesia):
The entrance gate is any area of the integument (usually the mucous membrane of the oropharynx and larynx). Following fixation of the bacterium, reproduction occurs at the site of introduction. Further, the production of exotoxin causes necrosis of the epithelium, tissue anesthesia, slowing of blood flow, and the formation of fibrinous films. Diphtheria microbes do not spread beyond the focus, but the toxin spreads through the connective tissue and causes dysfunction of various organs:
1. According to clinical form:
a) atypical (catarrhal);
b) typical (with films):
2. By severity:
3. By carrier:
4. By localization:
5. For diphtheria of the pharynx:
a) atypical;
b) typical:
6. By the nature of inflammation:

It is carried out in a hospital setting (mild forms may be unrecognized and treated at home).
It is most effective to start therapy in the first three days of the disease. The regime in the hospital is boxed, bed (as there is a risk of developing heart paralysis). The time limit for localized diphtheria is 10 days, for toxic diphtheria – 30 days, for other forms – 15 days.
Diet No. 2 according to Pevzner at the height of the disease (mechanically and chemically gentle, complete composition), then diet No. 15 (common table).
At the very first time, the administration of anti-diphtheria serum (i.m. or i.v.) after the test is indicated:
An integral part of treatment is antibiotic therapy (antibiotics of the penicillin, aminopenicillin, cephalosporin series).
Pathogenetic therapy includes detoxification and hormonal support if necessary.
The following groups of drugs can be used as symptomatic therapy:
Treatment of carriers is carried out using antibiotics according to general principles.
Rules for discharge of patients:
After discharge from the hospital, final disinfection is carried out in the box.
The most important way to prevent severe forms of diphtheria infection worldwide is through vaccination. The primary course is carried out in childhood, followed by regular revaccinations in adulthood (every 10 years). Vaccination saves not from bacterial carriage, but from the toxin produced by the bacterium, which causes a severe clinical picture. In this light, the need to constantly maintain a protective level of antitoxic immunity and regularly carry out revaccination (in the Russian Federation - with the ADS-m vaccine) becomes clear.
Diphtheria is an acute infectious disease that is life-threatening. It occurs in the form of acute inflammation of the upper respiratory tract, mainly the pharynx (approximately 90% of cases), nose, skin in places where it is damaged, eyes or genitals.
The main threat, however, is not inflammation, but poisoning with a toxin produced by the bacteria that causes the disease, which primarily affects the cardiovascular and nervous systems.
The causative agent of diphtheria is Corynebacterium diphteriae– gram-positive bacteria in the form of rods with characteristic flask-shaped thickenings at the ends, which in smears are arranged in pairs, at an angle in the form of a Roman numeral V relative to each other. During their life processes, diphtheria bacilli secrete diphtheria toxin, neuraminidase enzyme and other biochemically active compounds.
The synthesis of diphtheria toxin by microbial cells is controlled by a special tox gene. Bacteria can lose it in the process of life, losing along with it their ability to produce a toxin (toxigenicity). Conversely, initially non-toxigenic strains can acquire pathogenic properties; fortunately, this happens extremely rarely.
The disease is transmitted by airborne droplets from patients with diphtheria or from healthy carriers of the infection, much less often - through household items.
Children aged 3–7 years are most susceptible to diphtheria infection, but in recent years the incidence has increased in adolescents and adults.
The source of infection is sick people or healthy carriers of toxigenic bacteria. Those suffering from diphtheria of the pharynx, nose and larynx are the most contagious, as they actively excrete pathogens with exhaled air. Patients with diphtheria of the eyes and skin can spread the infection through contact (hands, household objects). Healthy carriers of bacteria are much less infectious, but their lack of any external signs of their condition does not allow us to control the spread of infection by them, because they can only be detected by chance during mass dispensary examinations. As a result, most cases of diphtheria infection are caused by contact with healthy carriers of the diphtheria bacillus.
The incubation period (the time from the moment of infection to the appearance of the first signs of the disease) is 2–10 days.
The toxin produced by the diphtheria bacillus consists of several components. One of them, the enzyme hyaluronidase, destroys hyaluronic acid in capillaries and increases their permeability, which leads to the release of blood vessels and saturation of surrounding tissues with blood plasma with the deposition of fibrinogen protein. The second component, necrotoxin, destroys epithelial cells and releases the enzyme thrombokinase from them. Thrombokinase promotes the conversion of fibrinogen into fibrin and the formation of a fibrin film on the surface of tissues. When diphtheria toxin acts on the palatine tonsils, which are covered with several layers of epithelial cells, a fibrin film is formed that penetrates deep into the epithelium of the tonsils and is tightly fused to it.
The third (main) component, the toxin itself, is capable of blocking the processes of cellular respiration and the synthesis of protein molecules. The most sensitive to its action are capillaries, myocardial cells and nerve cells. As a result, myocardial dystrophy and infectious-toxic myocarditis develop, damage to capillaries leads to infectious-toxic shock, damage to Schwann cells (auxiliary cells of nerve tissue) leads to demyelination of nerve fibers (destruction of the electrically insulating layer of myelin with disruption of the conduction of nerve impulses along nerve fibers). In addition, diphtheria toxin causes general intoxication of the body.
Diphtheria pharynx usually begins with a slight increase in temperature, slight pain when swallowing, redness and swelling of the tonsils, the formation of a specific filmy coating on them, and enlargement of the anterior upper cervical lymph nodes. The color of the films is usually white in the first 2–3 days of the disease, but then becomes gray or yellowish-gray. After about a week, the disease either ends with recovery (a mild form, as a rule, in those vaccinated against diphtheria), or turns into a more severe toxic form caused by the systemic action of diphtheria toxin.
The toxic form of diphtheria is always very difficult. It is characterized by very high body temperature (39.5-41.0°C), severe headaches, drowsiness, and apathy. The skin becomes pale, the mouth becomes dry, and children may experience repeated vomiting and abdominal pain. Swelling of the tonsils becomes pronounced, can lead to complete closure of the entrance to the pharynx, spreads to the soft and hard palate, often also to the nasopharynx, breathing becomes difficult, the voice often becomes nasal. The plaque spreads to all tissues of the oropharynx. A classic sign of the toxic form of pharynx diphtheria is swelling of the subcutaneous tissue in the neck and sometimes chest, resulting in the skin acquiring a gelatinous consistency. The anterior upper cervical lymph nodes are significantly enlarged and painful.
Nasal diphtheria occurs against the background of normal or slightly elevated body temperature, there is no intoxication. Serous-purulent or bloody-purulent discharge is visible from the nasal passages. Weeping areas and then dry crusts appear on the wings of the nose, cheeks, forehead and chin. Filmy deposits are visible inside the nose. The pathological process can also affect the paranasal sinuses. In the toxic form, swelling of the subcutaneous tissue of the cheeks and neck is observed.
Diphtheria eyes proceeds as a banal conjunctivitis and is characterized by moderate hyperemia and swelling of the conjunctiva of the eyelid, a small amount of serous-purulent discharge from the conjunctival sac (catarrhal form). The membranous form is manifested by pronounced swelling of the eyelids and the presence of greyish-white films on their conjunctiva that are difficult to remove. The toxic form is also accompanied by swelling of the tissue around the orbit.
Skin diphtheria leads to prolonged non-healing of any skin damage, hyperemia, a dirty gray coating is present on the skin, and dense infiltration of the surrounding skin is noted.
Diphtheria is diagnosed based on examination of the patient and test results. Upon examination, the diagnosis of diphtheria is indicated by the following signs: the presence of characteristic films, as well as difficulty breathing and a whistling noise when inhaling, not characteristic of a sore throat, a barking cough. The diagnosis of diphtheria based on characteristic clinical signs in a mild form of the disease is more difficult to make.
Analyzes:
A general blood test shows signs of an acute inflammatory process.
Examination of a smear under a microscope (bacterioscopy) - identification of bacteria with a characteristic appearance Corynebacterium diphteriae.
Bacteriological research is the inoculation of biological material on a special nutrient medium and the cultivation of colonies of microorganisms.
Determination of the level (titer) of antitoxic antibodies (a high titer of 0.05 IU/ml and above allows diphtheria to be excluded).
Serological study - determination of specific antibodies in blood serum using the methods of RPGA, ELISA, etc.
Diphtheria of the pharynx must be differentiated from acute tonsillitis (follicular and lacunar forms), Simanovsky-Vincent angina (fungal infection), syphilitic angina, pseudofilm angina with infectious mononucleosis, paratonsillar abscess, mumps, leukemia. In children, the diagnosis of false croup should be avoided.
All patients with diphtheria, regardless of the severity of the condition, must be hospitalized in an infectious diseases hospital.
Treatment is as follows:
Diet – fortified, high-calorie, thoroughly cooked food.
Etiotropic therapy (that is, aimed at eliminating the cause of the disease) - administration of anti-diphtheria serum (ADS), the dose and number of times of administration depend on the severity and form of the disease. In mild forms, PDS is administered intramuscularly once at a dose of 20–40 thousand IU; in moderate forms, 50–80 thousand IU is administered once or, if necessary, again in the same dose after 24 hours. When treating a severe form of the disease, the total dose increases to 90–120 thousand IU or even 150 thousand IU (infectious-toxic shock, disseminated intravascular coagulation syndrome). In this case, 2/3 of the dose is administered immediately, and during the first day of hospitalization, 3/4 of the total dose should be administered.
Antibiotics: for mild forms - erythromycin, rifampicin orally, for moderate and severe forms - injection of penicillins or cephalosporins. Course duration is 10–14 days. Antibiotics do not affect diphtheria toxin, but they reduce the number of bacteria that produce it.
Local treatment - rinsing and irrigation with disinfectant solutions.
Detoxification therapy - glucose-saline solutions, taking into account the daily need for fluid and its losses (moderate and severe forms).
Glucocorticosteroids – for moderate and severe forms.
Treatment of bacteria carriers is carried out with antibiotics: tetracyclines (children over 9 years old), erythromycin, cephalosporins against the background of general restorative therapy and elimination of chronic foci of infection.
Among the most serious complications of diphtheria on the cardiovascular system are myocarditis and heart rhythm disturbances.
Neurological complications of diphtheria are caused by damage to various cranial and peripheral nerves and are manifested by paralysis of accommodation, strabismus, paresis of the limbs, and in more severe cases, paralysis of the respiratory muscles and muscles of the diaphragm.
Secondary complications of diphtheria are such severe pathological conditions as acute cerebrovascular accidents (thrombosis, embolism), metabolic encephalopathy, cerebral edema, toxic kidney damage, diphtheria hepatitis, as well as infectious toxic shock and disseminated intravascular coagulation syndrome (disseminated intravascular coagulation syndrome - severe disorder of the blood coagulation system). The toxic form of diphtheria can lead to acute renal, cardiovascular, respiratory or multiple organ failure.
Nonspecific complications of diphtheria are peritonsillar abscess, otitis media, and pneumonia.
Vaccination against diphtheria is carried out with toxoid, that is, an inactivated toxin. In response to its administration, antibodies are formed in the body not to Corynebacterium diphteriae, but to diphtheria toxin.
Diphtheria toxoid is part of the combined domestic vaccines DTP (associated, that is, complex, vaccine against whooping cough, diphtheria and tetanus), AaDPT (vaccine with an acellular pertussis component) and ADS (diphtheria-tetanus toxoid), as well as “sparing” vaccines ADS-M and AD-M. In addition, the SanofiPasteur vaccines are registered in Russia: Tetracok (against diphtheria, tetanus, whooping cough, polio) and Tetraxim (against diphtheria, tetanus, whooping cough, polio, with an acellular pertussis component); D.T. Vax (diphtheria-tetanus toxoid for vaccination of children under 6 years of age) and Imovax D.T. Adult (diphtheria-tetanus toxoid for vaccination of children over 6 years of age and adults), as well as Pentaxim (vaccine against diphtheria, tetanus, whooping cough, polio and Haemophilus influenzae infection with an acellular pertussis component).
According to the Russian vaccination calendar, vaccination of children under one year of age is carried out at 3, 4–5 and 6 months. The first revaccination is carried out at 18 months, the second at 7 years, the third at 14. Adults should be revaccinated against tetanus and diphtheria every 10 years.
Diphtheria is an infectious disease provoked by exposure to a specific bacterium, the transmission of which (infection) is carried out by airborne droplets. Diphtheria, the symptoms of which are the activation of the inflammatory process mainly in the nasopharynx and oropharynx, is also characterized by concomitant manifestations in the form of general intoxication and a number of lesions that directly affect the excretory, nervous and cardiovascular systems.
In addition to the listed variants of damage, diphtheria can also manifest itself in its own benign form, which, accordingly, is accompanied by damage to the nose and the absence of pronounced manifestations characteristic of intoxication.
Inflammation, which is relevant for diphtheria, occurs in combination with a process such as the appearance of fibrin films that look like a white coating, and if we are, again, not talking about a benign form of the disease, then general intoxication additionally manifests itself.
Loeffler's bacillus was isolated as the causative agent of the disease. Its peculiarity lies, first of all, in a significant degree of resistance to the conditions of influence from the external environment. Thus, standard conditions determine such resistance for the pathogen for a period of within 15 days, resistance to exposure to low temperatures can be about 5 months, but resistance when in an aquatic environment or in milk is about three weeks. Death within one minute is achieved by boiling the pathogen or by treating it using a disinfectant solution (chlorine).
The source of the spread of infection is a sick person or a carrier of a toxigenic sample strain (in this case, a certain type of pathogen that provokes the development of the disease is implied). In the spread of infection, the greatest significance is determined for patients with oropharyngeal diphtheria identified in them, especially if we are talking about an erased form of the disease or its atypical form. A significant danger has also been identified for bacteria carriers whose pathogens are excreted through the oropharynx. Depending on the specific group of patients, long-term carriage of the infection in frequency ranges from 13-29%. Due to the continuity characteristic of the epidemic process, carriage is defined as long-term, even without the possibility of recording general morbidity.
The route of transmission of infection is airborne, while the transmission mechanism is aerosol. In some cases, variants in the form of objects used in environmental conditions (dishes, toys, clothes and linen, etc.) are considered as transmission factors. If the causative agent of the disease is on your hands, then the development of such forms of diphtheria as eye diphtheria, genital diphtheria and skin diphtheria is allowed - the specific option, as you can understand, is determined on the basis of further spread. In addition, the route of food contamination is also possible, for example, when the virus multiplies in confectionery cream, in milk, etc.
If we talk about natural susceptibility to infection, it is quite high and is determined on the basis of the current antitoxic immunity of each individual patient. For example, if the blood contains specific antibodies in an amount of about 0.03 AE/ml, then protection against diphtheria is considered as a possibility, which, however, does not exclude the possibility of obtaining the status of a carrier of a pathogenic agent. Transplacental transfer of antitoxic antibodies to newborns ensures their protection against diphtheria during the first 6 months after birth.
As for patients who have had diphtheria, as well as patients who have undergone the correct vaccination procedure, they develop antitoxic immunity, which, due to its own level, determines a reliable degree of protection from subsequent possible exposure to the infection we are considering.
For diphtheria, the traditional autumn-winter seasonality for many diseases has been determined, although variants of the frequency of epidemics in which the cause of their occurrence is negligence in relation to prevention through vaccination are not excluded. Cases of negligence can occur both on the part of medical personnel and on the part of the population. The explanation for this is the increase in the number of people who have lost antitoxic immunity, which is acquired through vaccination or repeated vaccination (re-vaccination). Thus, the following causes of diphtheria can be identified as factors causing infection:
It is argued that diphtheria as a disease is subject to successful control, which is achieved, in particular, through vaccination of the population. In European countries, the beginning of mass immunization programs was noted in the 40s, due to which a rapid decrease in the incidence rate was revealed, down to single diagnosed cases in a number of countries. What is noteworthy is that with a significant decrease in the immune layer, the incidence rate increases accordingly. Involvement in epidemiological processes is noted not only for adult groups of the population, but also for children, in particular, this applies to cases with unreasonable withdrawals from the need for preventive vaccination, as a result of which the transmission of the pathogen from adults occurs due to their lack of the antitoxic immunity required to avoid this .
A separate point is assigned to the increased migration among the population in recent years, due to which the spread of the pathogen has increased. Already noted autumn-winter outbreaks of the disease (in other words, intra-annual morbidity), as well as periodic outbreaks (due to long-term dynamics), especially reach their peak when there are current defects in preventive vaccination.
Such conditions also dictate the possibility of a “shift” from childhood to an older age, with a predominant defeat of those individuals whose professional activities are most predisposed to infection (trade and transport workers, service workers, teachers, health workers, etc.) . Due to the sharp deterioration of the general epidemiological situation, the course of the disease is more severe, as a result of which the risks in terms of mortality associated with the disease also increase.
The main gates for infection to enter the body are the mucous membranes of the oropharynx, and, somewhat less frequently, the mucous membranes of the larynx and nose. Also, as highlighted above, the possibility of damage to the ears, conjunctiva, skin and genitals is possible. Toxigenic strains of bacteria secrete enzymes and exotoxin, due to the influence of which foci of inflammation are subsequently formed.
Features of the local effects produced by diphtheria toxin are non-coagulative necrotic processes in the epithelium, vascular hyperemia (overflow of blood within a certain organ or part of the body), as well as blood stasis (slowing down blood flow and stopping it) in the capillaries and increasing the degree of permeability of vessel walls. Exudate (a turbid liquid saturated with hematogenous and histogenic cells and protein that sweats from blood vessels at the site of inflammation), the composition of which also includes macrophages, leukocytes, fibrinogen and erythrocytes, leaves the normal vascular bed. Subsequently, fibrinogen, under the influence of a reaction against the background of contact of the mucosa with thromboplastin (related to tissues that have undergone necrotization), is converted into fibrin.
Next, fibrin, or rather the fibrin film, begins to densely concentrate and fixate on the epithelium of the pharynx and pharynx. During this period, it is easily eliminated from the mucous membrane based on single-layer epithelium in the bronchi, trachea and larynx. At the same time, the mild course of diphtheria may be limited only to the development of the usual catarrhal process, not accompanied by the appearance of fibrinous plaque.
However, the further picture of the course of the disease may look like this. Neuraminidase of the causative agent of diphtheria (a specific glycoprotein complex, due to which enzymatic activity is ensured, which, in turn, determines the ability of a viral particle to penetrate the host cell with its subsequent exit after reproduction) has a pronounced potentiating effect on the exotoxin. Its main part is histotoxin, which blocks the process of synthesis in cells of protein and transferase, which acts as an inactivating enzyme and is responsible for the formation of polypeptide bonds.
Diphtheria exotoxin spreads through the blood vessels and lymph nodes, which, in turn, determines the conditions for the development of intoxication with its corresponding symptoms, as well as the conditions for the development of regional lymphadenitis in combination with swelling of the tissues located in the immediate environment of the affected environment. Severe cases lead to the fact that swelling of the tonsils, palatine arches and uvula causes the development of swelling of all tissue concentrated in the neck; the degree of swelling in this case corresponds to the specific stage of the disease.
Due to the current process of toxinemia (a condition accompanied by the circulation of bacterial exotoxin through the circulatory system with its delivery to the so-called target cells), inflammatory-degenerative processes and microcirculatory disorders develop in various systems and organs (nervous and cardiovascular systems, adrenal glands and kidneys).
The process of binding of the toxin and specific cellular receptors occurs in accordance with two phase options, in particular, these are reversible and irreversible phases. Reversible phase makes it possible to maintain cell viability while at the same time allowing for the possibility of neutralizing the toxin due to antitoxic antibodies. Concerning irreversible phase, then here, accordingly, neutralization of the toxin due to antibodies does not occur, therefore there are no obstacles to the implementation of the cytopathogenic activity it produces.
To complete the consideration of this section, which to some extent clarifies the features of the course of the disease, we will add that the antitoxic immunity that develops in a patient against the background of diphtheria does not always act as sufficient protection to further prevent this disease from occurring again when infected with the pathogen.
The duration of the incubation period (i.e., the period that lasts from the moment of infection until the moment the first symptoms relevant to the disease appear) is about 2-10 days. During these days, in the area of the entrance gate of infection (respiratory tract, genitals, oropharynx, skin or eyes), the diphtheria pathogen enters the body. At the same time, when diphtheria bacteria come into contact with epithelial cells, they begin to provoke cell separation in tissues, which is achieved by suppressing the synthesis process in their protein fractions (the so-called “line of first defense”; it is this line that is affected).
In parallel, in accordance with the picture of the pathogenesis of diphtheria discussed above, the exotoxin begins to have a corresponding effect, due to which the tissues are killed, edema develops and intercellular fluid (exudate) appears, which is subsequently converted into fibrin. Fibrin appears externally as a yellowish film (plaque) covering the mucous membranes.
The classification of diphtheria determines a number of forms of this disease, which, in turn, are characterized by their own characteristics of the course. Oropharyngeal diphtheria, which is listed first on the list, is most often diagnosed.
Below we will look at the symptoms and features of each option.
This form of diphtheria is diagnosed in approximately 90-95% of cases, both for diphtheria in adults and children. In approximately 75% of cases, its course is localized.
The onset of the disease in this form is characterized by the severity of its own manifestations, patients’ temperature rises (from values ranging from 37.5 degrees to higher), the duration of its persistence is about 3 days. The severity of intoxication manifestations is characterized by moderation; we recall that these manifestations include headache, pale skin, decreased appetite, increased heart rate and general malaise. A further decrease in temperature is countered, on the contrary, by the activation of manifestations from the entrance gates of infection, which not only persist, but can also gradually increase in intensity.
The severity of pain in the throat, noted when swallowing, is determined on the basis of current changes in the oropharynx, where there is a diffuse and mild form of hyperemia, moderate swelling in the tonsils, arches and soft palate. Localization of plaques is noted only on the side of the tonsils; in this case, they do not go beyond their boundaries; the location of these plaques is carried out either in the form of separate islands or in the form of a filmy layer.
In the first hours after the onset of the disease, filmy plaques resemble a jelly-like mass in consistency, after which they transform into a cobweb-like thin film. From the second day of its appearance, this film acquires pronounced density and smoothness, and its color also changes (to grayish with a pearlescent sheen). Such a film is removed with difficulty, after which the surface of the mucous membrane bleeds. By the next day after removing the film, a new layer of film will form. If such a film is placed in water after removal, you will notice that it does not sink and is not subject to separation and disintegration.
The localized form of diphtheria is accompanied by the formation of typical fibrinous plaques in approximately a third of cases of this disease in adults, while in other cases (including when considering later periods of manifestation of the disease, 3-5 days), the plaques are characterized by looseness and ease of removal, while Removal is accompanied by a virtual absence of mucosal bleeding. There is also a moderate increase in regional lymph nodes and submandibular lymph nodes; they are sensitive to palpation. Actual processes in the tonsil area, as well as the reaction following from the regional lymph nodes, can be one-sided and asymmetrical.
At catarrhal variant manifestations of a localized form of oropharyngeal diphtheria, a minimum of local and general symptoms are noted. However, this form is diagnosed quite rarely. Here, there is a normal or short-term subfebrile temperature (up to 37.5 degrees) and mild symptoms characteristic of intoxication, which also occur in combination with unpleasant sensations that occur in the throat when swallowing. The tonsils are swollen, the oropharynx is subject to a mild form of hyperemia. Diphtheria as a diagnosis in this case can be considered only on the basis of taking into account the patient’s anamnesis (medical history) in combination with the results of laboratory examinations and taking into account the characteristics of the general epidemiological situation.
As a rule, this form is characterized by its own good quality. Following the normalization of the temperature, the pain that appears in the throat when swallowing disappears; the duration of plaque on the tonsils can be about 8 days. Meanwhile, if you ignore the need to treat oropharyngeal diphtheria, then the possibility of disease progression cannot be ruled out, and, even worse, the possibility of transformation into more severe forms.
Diphtheria of the oropharynx in its common form diagnosed relatively rarely - in approximately 3-11% of diphtheria cases. The difference from the localized form lies in the widespread nature of the manifestation of plaque, moving beyond the tonsils to any areas located in the area of the oropharyngeal mucosa. The nature of the symptoms (swelling of the tonsils, intoxication, enlargement and pain of the lymph nodes of the submandibular region) has a more pronounced form (compared to the localized form). Edema of the cervical subcutaneous tissue does not develop in this case.
Next, subtoxic form of diphtheria of the oropharynx area, characterized by the manifestation of intoxication and severe pain noted in the throat when swallowing. In some cases, pain manifests itself in the neck area. A characteristic plaque appears on the tonsils (it is localized in nature, spreading only slightly to the uvula and palatine arches), the tonsils themselves change in color (become purple-bluish). Swelling (uvula, arches, soft palate and tonsils) is moderate, regional lymph nodes are compacted. This form of diphtheria has a characteristic feature; it consists in the development of edema in the area above the regional lymph nodes, often this edema is one-sided.
Further - toxic form of oropharyngeal diphtheria. Now it is diagnosed quite often (in approximately 20% of cases of general morbidity), diphtheria in adults in this form is especially relevant. It develops either because of an untreated localized form of the disease or because of its widespread form, although in the vast majority of cases, spontaneous independent development of the disease is observed with its subsequent rapid progression.
As a rule, patients are diagnosed with a high temperature (within 39-41 degrees), and it occurs already in the first hours of the disease. In addition to this, other symptoms of intoxication arise, and these are weakness and headache, these manifestations are also accompanied by severe pain in the throat, in some cases - pain in the abdomen and neck. The possibility of vomiting and the development of a disorder of the masticatory muscles such as painful trismus (restrictions in opening the mouth) cannot be ruled out.
Delirium (a form of mental disorder accompanied by impaired consciousness), excessive agitation, delirium and euphoria may develop. In addition, pallor of the skin is noted (III degree of the toxic form of the disease can manifest itself in the form of hyperemia, that is, redness of the facial skin). Severe edema in combination with diffuse hyperemia of the oropharyngeal mucosa within the II and III degrees is accompanied by complete closure of the lumen of the pharynx, which is considered as a precursor to the formation of fibrinous plaque.
The spread of plaque in this case occurs rapidly, to each of the sections of the oropharynx. Subsequently, such films thicken and become coarser; their retention period on the mucosal surface is on average 2 weeks, although a longer period for this manifestation is allowed. Often the process is one-sided, the enlargement of regional lymph nodes occurs early, to a significant size, their soreness and density are also noted, and the tissues surrounding them gradually become inflamed (periadenitis).
The peculiarities of local manifestations that are relevant in this toxic form of the disease distinguish it from other forms in that a painless pasty swelling is formed in the cervical subcutaneous tissue. I degree of diphtheria here is accompanied by reaching the area of the middle of the neck, II degree is accompanied by a similar lesion of the collarbone, and III degree occurs with a characteristic lesion of the collarbone going downwards, and the spread of the lesion can affect the back of the neck, back and face, all this occurs with the gradual progression of the disease.
The general toxic syndrome has a pronounced manifestation pattern, with increased heart rate, cyanosis of the lips, and low blood pressure. The temperature also rises, and if it decreases, the manifestations of other symptoms still remain pronounced. A characteristic feature in this case is a specific type of sickly putrid smell and a nasal voice. Often, toxic diphtheria is accompanied by the addition of lesions of the nose and larynx; in this case, the form, as is clear, is combined, characterized by the severity of its own course and the difficulty of influencing therapeutic measures against it.
The most severe form of diphtheria is its hypertoxic form. Basically, this course of diphtheria is diagnosed in patients with a relevant negative premorbid background (that is, with concomitant alcoholism, chronic hepatitis, diabetes, etc.). Symptoms of diphtheria consist, first of all, in a rapid increase in temperature, and the temperature in this case is accompanied by chills and a pronounced form of intoxication in its corresponding manifestations (headache, dizziness, general malaise and vomiting). In addition to this, progressive forms of hemodynamic disorders are also noted, which manifests itself in the form of rapid heartbeat, pale skin, and low blood pressure.
Skin hemorrhages also appear, bleeding from internal organs is urgent, fibrinous deposits become saturated with blood (DIC syndrome develops). The clinic is characterized by a dominant state of signs accompanying the development of an infectious-toxic form of shock, and this, in turn, can lead to death within 1-2 days from the onset of the disease, which, accordingly, indicates the inadmissibility of any delays in parts of treatment for these symptoms.
This form of the disease can occur in a localized form (the larynx is affected, respectively, this is laryngeal diphtheria) or in a widespread form (the larynx, trachea, and sometimes the bronchi are simultaneously affected).
If the variant of the common form is considered, then here it is mainly noted that it is combined with diphtheria of the nose and oropharynx. It should be noted that symptoms of diphtheria in adults have recently occurred in this form quite often. Features of the manifestation of croup consist in alternately following three stages of the flow. So, this is the dysphonic stage, the stenotic stage and the asphyxial stage. Manifestations of intoxication in all cases are characterized by their own moderation.
As leading manifestations corresponding dysphonic stage, there is a barking cough in the rough form of its own manifestation, as well as an increase in hoarseness. Symptoms of diphtheria in children at this stage appear within 1-3 days, while adults endure it somewhat longer - up to 7 days.
Next, stenotic stage, characterized by a duration of up to 3 days. The patient's voice loses its sonority (turns to a whisper), the cough manifests itself silently. The patient's pallor and restlessness are noted. Breathing is noisy, inhalation is prolonged, signs indicating difficulty breathing gradually increase. The skin and mucous membranes are characterized by pallor and cyanosis, and the heartbeat also increases. With an increase in the listed signs, the question arises about the need to provide tracheostomy or intubation, due to which it is possible to prevent the progression of the disease to the next stage.
The next stage is asphyxial stage, it is accompanied by shallowness and rapidity of the patient’s breathing, which subsequently becomes rhythmic. The blueness of the skin and mucous membranes gradually increases, blood pressure decreases, and the pulse is thready. Further, there is a disturbance of consciousness, the occurrence of convulsions and, ultimately, death occurs due to asphyxia (suffocation, accompanied by a lack of oxygen in the tissues and blood with the simultaneous accumulation of carbon dioxide in them).
Considering the anatomical features of the larynx in adults (compared to the larynx in children), the development of diphtheria croup in them requires more time than its development in children. What is noteworthy is that in a certain proportion of cases the course of the disease occurs only with concomitant hoarseness, combined with a feeling of lack of air. Additionally, you should pay attention to pale skin, increased heart rate, and decreased breathing. Making a diagnosis in this case is facilitated by performing a laryngoscopic or bronchoscopic examination, which makes it possible to detect hyperemia of the larynx and its swelling, the ability to study the characteristics of membranous formations in the vocal cords, as well as the characteristics of damage to the bronchi and trachea as part of the course of the disease.
The disease in this form is characterized by a slight degree of intoxication, the appearance of serous-purulent discharge or ichor-type discharge, and difficulty in nasal breathing. There is redness of the nasal mucosa, swelling and the appearance on its surface of ulcers, erosive formations or fibrinous film deposits resembling “shreds”. In the area surrounding the nose, irritation develops, weeping is also noted in combination with crusts that form here, and in this form of the disease a runny nose persists. As a rule, nasal diphtheria occurs in combination with another type of diphtheria lesions, that is, with diphtheria of the larynx and/or oropharynx, in some cases with diphtheria of the eyes, the features of which we will consider below.
This form of diphtheria, in turn, occurs in a catarrhal, membranous and toxic form.
Catarrhal form is characterized predominantly by unilateral inflammation of the conjunctiva, which is accompanied by the appearance of a certain amount of eye discharge. The temperature, as a rule, either does not change or reaches the limits of subfebrile indicators (up to 37.5 degrees). In this case, there is no regional inflammation and enlargement of the lymph nodes, as well as no symptoms of intoxication.
Membranous form eye diphtheria is accompanied by mild general toxic symptoms in combination with low-grade fever; this is also accompanied by the formation of a fibrin film on the conjunctiva that has undergone redness. Additionally, swelling of the eyelids increases, and serous-purulent eye discharge appears. Initially, the process may manifest itself unilaterally, but after a few days the possibility of its subsequent transfer to another eye, that is, to the healthy eye, is allowed.
And finally toxic form diphtheria, accompanied by an acute onset and subsequent rapid development of intoxication symptoms. The eyelids swell, profuse purulent eye discharge appears, the skin around the eye is subject to weeping and general irritation. As the disease progresses, edema gradually spreads, causing the subcutaneous tissue in the facial area to be affected. Often this form of the disease is accompanied by damage to other parts of the eye, which can even reach panophthalmia (inflammation of the eyeball); regional inflammation of the lymph nodes in combination with their soreness also manifests itself.
The listed variants of manifestation of diphtheria are diagnosed quite rarely. As a rule, they develop in combination with other forms of diphtheria, for example, with nasal diphtheria or with diphtheria of the pharynx. As general features of these options, one can note the manifestations common to diphtheria in general, and these are swelling, oozing, hyperemia of the skin and mucous membranes, the appearance of fibrinous plaque in the affected area, inflammation and soreness of regional lymph nodes.
Diphtheria of the genital organs in men is accompanied by a concentration of the pathological process within the foreskin. As for diphtheria of the genital organs in women, here it may have a more common form of course, accompanied by the process involving the perineum, vagina and labia, as well as the anus, while serous-bloody discharge coming from the genital tract is considered as concomitant manifestations . Urination becomes difficult, and this process is also accompanied by pain.
Skin diphtheria also has its own characteristics, which is characterized by the development of a pathological process in the area of concentration of diaper rash, wounds, eczema or fungal lesions in combination with visible cracks in the skin with the formation of a dirty gray plaque and the release of serous-purulent exudate. As for traditional general toxic manifestations, in this case they are insignificant; regression of the local process occurs slowly (a month or longer).
Traumatization of the skin or mucous membranes, which is subsequently accompanied by the introduction of the pathogen, is considered as a predisposing factor to the development of the forms of diphtheria indicated in this paragraph.

The diagnosis of diphtheria is largely clinical, which allows it to be established on the basis of a visual examination. As for additional diagnostic methods, they are also used - this is done in particular to diagnose atypical forms of the disease, to determine specific strains, and also to deregister a patient for a given diagnosis.
Laboratory diagnostic methods:
The need for diagnostics regarding possible complications is considered as a separate point. So, in case of suspicion of carditis, an ultrasound of the heart, phonocardiography, and ECG are performed, in addition, the characteristics of the activity of aspartate aminotransferase, creatine phosphokinase and lactate dehydrogenase are examined. If there is a suspicion of nephrosis that is relevant to the patient, then the following diagnostic procedures are performed: biochemical blood test (for urea and creatinine levels), kidney ultrasound, CBC and OAM.
Treatment of diphtheria is based on a number of the following basic principles:
In hospitals, intensive care units and intensive care units, the following additional treatment measures can be implemented:
It is mandatory to prescribe three weeks of bed rest (a condition subject to strict adherence). In the future, it is necessary to register for this disease with a cardiologist - this will provide the opportunity to diagnose complications in this profile in the late form of their manifestation with an actual connection with diphtheria. A gentle diet for diphtheria is prescribed, taking into account the need to reduce hypoallergenic foods.
Complications of diphtheria may include myocarditis, as well as dysfunction of the nervous system, which usually manifests itself as paralysis. Diphtheria is often complicated by the development of paralysis of the soft palate, neck muscles, respiratory tract, vocal cords, and limbs. It should be noted that paralysis of the respiratory tract can lead to asphyxia (which is important for croup), which, as we have already indicated, can lead to death.
If symptoms appear that correspond to the course of diphtheria, it is necessary to contact the attending physician and infectious disease specialist; in the future, the patient can be registered with a cardiologist.
Is everything in the article correct from a medical point of view?
Answer only if you have proven medical knowledge
RCHR (Republican Center for Health Development of the Ministry of Health of the Republic of Kazakhstan)
Version: Clinical protocols of the Ministry of Health of the Republic of Kazakhstan - 2017
Diphtheria (A36), Diphtheria, unspecified (A36.9)
Approved
Joint Commission on Healthcare Quality
Ministry of Health of the Republic of Kazakhstan
dated May 12, 2017
Protocol No. 22
Diphtheria- an acute anthroponotic infectious disease with an aerosol transmission mechanism of the pathogen, characterized by predominant damage to the oropharynx and respiratory tract with the development of fibrinous inflammation at the site of introduction of the pathogen and toxic damage to the cardiovascular system, nervous system and kidneys.
INTRODUCTORY PART
ICD-10 code(s):
Date of development of the protocol: 2017
Abbreviations used in the protocol:
| GP | - | general doctor |
| GOTH | - | glutamate oxaloacetate transaminase |
| ITS | - | infectious-toxic shock |
| ELISA | - | linked immunosorbent assay |
| KIZ | - | office of infectious diseases |
| KFC | - | creatine phosphokinase |
| LDH | - | lactate dehydrogenase |
| UAC | - | general blood analysis |
| OAM | - | general urine analysis |
| surge arrester | - | acute renal failure |
| PDS | - | anti-diphtheria serum |
| PHC | - | primary health care |
| REEF | - | immunofluorescence reaction |
| RLA | - | latex agglutination reaction |
| RNGA | - | indirect hemagglutination reaction |
| RPGA | - | passive hemagglutination reaction |
| ESR | - | erythrocyte sedimentation rate |
| Ultrasound | - | ultrasonography |
| ECG | - | electrocardiography |
Level of evidence scale:
| A | A high-quality meta-analysis, systematic review of RCTs, or large RCTs with a very low probability (++) of bias, the results of which can be generalized to an appropriate population. |
| IN | High-quality (++) systematic review of cohort or case-control studies or high-quality (++) cohort or case-control studies with very low risk of bias or RCTs with low (+) risk of bias, the results of which can be generalized to the relevant population . |
| WITH | Cohort or case-control study or controlled trial without randomization with a low risk of bias (+), the results of which can be generalized to the relevant population or RCT with a very low or low risk of bias (++ or +), the results of which cannot be directly distributed to the relevant population. |
| D | Case series or uncontrolled study or expert opinion. |
| GPP | Best clinical practice. |
Classification
By process localization:
Diphtheria of the oropharynx (pharynx);
- localized (island, filmy);
- widespread;
- toxic (subtoxic, toxic I, II, III degrees, hypertoxic);
Diphtheria of the respiratory tract:
- diphtheria of the larynx (localized diphtheria croup);
- widespread diphtheria croup (diphtheria laryngotracheobronchitis);
Nasal diphtheria;
diphtheria of the eye;
Diphtheria of the genital organs;
skin diphtheria;
· combined form of diphtheria.
By severity:
· light;
· medium-heavy;
· heavy.
DIAGNOSTIC METHODS, APPROACHES AND PROCEDURES
Diagnostic criteria:
Complaints and anamnesis:
Non-toxic forms of diphtheria oropharynx begins with moderately severe symptoms of intoxication:
lethargy;
· temperature increase (up to 38-39°C for 2-4 days);
· sore throat, mainly when swallowing;
· headache;
· pallor of the skin.
Llocalized diphtheria of the oropharynx- fibrinous deposits do not extend beyond the palatine tonsils:
with island form
in the oropharynx it is noted:
· enlargement, swelling of the tonsils and palatine arches;
· mild hyperemia with a cyanotic tint;
· formation of fibrinous effusion in the depths of the crypts and on the convex surface of the tonsils;
· edema prevails over infiltration, leading to a uniform spherical enlargement of the tonsils and smoothness of their surface structure.
with filmy form
:
· At first, the deposits look like a translucent pink film;
· then soaked in fibrin;
· by the end of the first, beginning of the second day they become fibrinous films with a smooth surface of a whitish-gray color and a pearlescent sheen;
· Subsequently, a thick film is formed, dense, often continuous, difficult to remove;
· in case of forced rejection, bleeding erosions are visible under the film on the surface of the tonsils;
· the film dropped into water does not dissolve, sinks and does not lose its shape, and does not rub on the glass;
· the duration of the raids is 6-8 days;
· submandibular (angular jaw, tonsillar) lymph nodes enlarge up to 1-2 cm, mild or painless, elastic.
Specific inflammation outside the tonsils on the uvula, soft palate, oral mucosa, intracanalicularly in the larynx, nasal cavity, more pronounced:
· swelling, hyperemia of the tonsils, palatine arches;
· enlargement of regional lymph nodes;
· painful sensations;
· the course is favorable;
· in 12.5% the development of complications in the form of mild polyneuropathies.
Diphtheria of the larynx- gradual onset;
· low-grade fever with mild general intoxication;
· absence of catarrhal phenomena.
Three stages of croup with laryngeal diphtheria:
1. Catarrhal stage (lobar cough)- a sharp, loud cough, which soon became rough, barking, and then lost its sonority, becoming hoarse.
2. Stage of stenosis (stenotic)- aphonia, silent cough, prolongation of inspiration, noisy breathing with retraction of the pliable parts of the chest, psychomotor agitation, increasing hypoxia.
3. Asphyxial stage- the tone of the respiratory center decreases, drowsiness and weakness appear. Breathing is rapid, but superficial, the extremities are cold, the pulse is frequent, thread-like, sometimes paradoxical. Death occurs as a result of exhaustion of the respiratory centers and circulatory disorders.
Toxic form of oropharyngeal diphtheria- acute development of symptoms:
· temperature rise to 39-40°C;
· headache;
· chills;
· severe general weakness;
· anorexia;
· pallor of the skin;
repeated vomiting;
· abdominal pain;
· periods of excitement are replaced by progressive adynamia;
· early spread of plaque beyond the tonsils;
· the appearance of an unpleasant, sugary-sweet odor from the mouth;
· regional lymph nodes are significantly enlarged and painful.
At subtoxic diphtheria of the oropharynx:
· plaque is limited to the tonsils or spread to the uvula, soft palate, back wall of the pharynx;
· swelling of the soft tissues of the oropharynx;
· swelling of the cervical tissue is one-sided, slightly widespread, mainly in the area of the lymph nodes.
For toxic diphtheria of the oropharynx
swelling of the subcutaneous tissue of the neck is characteristic, of a pasty consistency, appears on the 2nd - 3rd day of the disease, spreads from the front down, then to the face, back of the head and back, the color of the skin above the swelling is not changed:
· swelling up to the middle of the neck - toxic form of 1st degree;
· spread of edema to the collarbone - 2 degrees;
· below the collarbone - toxic form of the 3rd degree.
Nasal diphtheria characterized by difficulty in nasal breathing:
· appearance of mucous, serous-mucosal, sanguineous nasal discharge;
· irritation of the wings of the nose and the skin of the upper lip;
· on the nasal mucosa there are typical diphtheritic films, sometimes erosions;
· filmy deposits can spread to the turbinates and the bottom of the nose;
· health is slightly disturbed;
· no intoxication;
· body temperature is normal or subfebrile;
· congestion of the nasal passages and sanguineous discharge from the nose for 2 - 3 weeks.
Diphtheria eye can be localized (affecting only the mucous membranes of the eyelids), widespread (affecting the eyeball) and toxic (with swelling of the subcutaneous tissue around the eyes):
· eyelids swell, become dense to the touch, and open with difficulty;
· discharge is serous-bloody, initially scanty, then abundant, after 3-5 days - purulent;
· on the connective membrane of the eyelids there are dirty-gray, tightly fitting plaques, swelling is pronounced;
· temperature rises;
· the patient’s well-being is disturbed;
· symptoms of intoxication are moderately expressed;
· In some cases, the cornea is affected, which leads to visual impairment.
Skin diphtheria It is more common in children of the first year of life, localized in skin folds - on the neck, in the groin folds, armpits, behind the ear.
Diphtheria of the external genitalia occurs predominantly in girls of preschool and school age.
Typical localized filmy form
- hyperemia with a cyanotic tint, fibrinous films, enlarged inguinal lymph nodes.
Common form
- the inflammatory process spreads to the perineum, the skin around the anus.
Toxic form
- swelling of the labia (1st degree), subcutaneous tissue of the groin areas, pubis and thighs (2nd -3rd degree).
Physical examination:
Localized forms:
oropharyngeal diphtheria:
· mild hyperemia of the oropharyngeal mucosa;
· moderate swelling of the tonsils and palatine arches;
· filmy plaques on the tonsils;
· moderately enlarged and slightly painful regional lymph nodes;
· plaques are uniformly fibrinous, at the beginning of formation;
loose cobweb-like or jelly-like (transparent or cloudy);
· easy to remove;
· formed deposits are dense;
· are removed with difficulty and bleeding.
diphtheria of the nasopharynx:
· enlargement of the posterior cervical lymph nodes;
· detection of fibrinous deposits during posterior rhinoscopy.
nasal diphtheria:
· bloody discharge, often unilateral;
· catarrhal-ulcerative inflammation or fibrinous films that initially appear on the nasal septum.
diphtheria of the eye:
· sharp swelling of the eyelids;
· copious mucopurulent discharge;
Conjunctival hyperemia;
· film on the conjunctiva of one or both eyelids.
genital diphtheria:
· catarrhal-ulcerative or fibrinous-necrotic urethritis or vulvitis.
Common forms:
oropharyngeal diphtheria:
· plaque spreads to the palatine arches, uvula, lower parts of the soft palate, lateral and posterior walls of the pharynx;
· moderate regional lymphadenitis;
There is no toxic swelling of the mucous membranes of the oropharynx and subcutaneous tissue of the neck.
nasal diphtheria:
· spread of plaque into the paranasal sinuses.
diphtheria of the eye:
· keratoconjunctivitis.
genital diphtheria:
· Plaques outside the vulva and glans penis.
Toxic forms:
oropharyngeal diphtheria
:
· toxic swelling of the mucous membranes of the oropharynx with maximum spread to the hard palate and laryngopharynx;
· color of mucous membranes - from bright hyperemia to sharp pallor, with cyanosis and a yellowish tint;
· extensive or limited hemorrhagic imbibition is possible, fibrinous plaques first form on the tonsils, then at the sites of toxic edema beyond them, in grade III and hypertoxic - with hemorrhagic impregnation;
· tonsillar lymph nodes are enlarged, painful and dense;
· temperature rise to 39-40 0 C;
· pallor;
· with toxic grade III and hypertoxic - delirious agitation with facial hyperemia.
Table 1. Criteria for determining a case of diphtheria [3
].
| Definition | Clinical criteria |
| Suspicious case | a): acute onset of the disease with fever, sore throat; tonsillitis, nasopharyngitis, or laryngitis with difficult-to-remove filmy deposits on the tonsils, pharyngeal wall and/or nasal cavity |
| Probable case | a) + b): a disease whose clinical picture corresponds to diphtheria |
| Confirmed case |
a) + b) + c): a probable case confirmed by laboratory methods (with the isolation of a toxigenic strain from the nose, oropharynx and other places where there may be deposits that occur with diphtheria) or epidemiologically linked to another laboratory-confirmed case of diphtheria |
Instrumental studies:
· ECG; EchoCG - changes indicate myocardial damage;
· X-ray of the chest organs;
· Ultrasound of the abdominal organs, kidneys;
· X-ray of the paranasal sinuses;
· Electroneuromyography;
· Laryngoscopy using video endoscopic technologies.
Indications for consultation with specialists:
· consultation with an infectious disease specialist, otolaryngologist to establish a preliminary diagnosis of diphtheria.
Algorithm for diphtheria diagnosis:
Differential diagnosis and rationale for additional studies [3
]
Table 2. Differential diagnosis of localized diphtheria of the oropharynx
| Clinical signs | Differentiable diseases | |||
| oropharyngeal diphtheria localized form | streptococcal sore throat | Infectious mononucleosis | Simanovsky-Vincent's angina | |
| Symptoms of intoxication | Moderate: lethargy, subfebrile temperature, sometimes rises to 38-39 0 C | Sharply expressed: acute onset, weakness, body aches, headache, body temperature up to 40 0 C | Weakly expressed, depending on the severity of the course | None. Subfebrile temperature |
| Appearance | Face pale | Facial hyperemia, shiny eyes, sometimes pale nasolabial triangle | The face is pale, puffy. Breathing through the nose is difficult | Ordinary |
| Timing of appearance of tonsillitis | 1-2 days. The process is often bilateral | End of 1st day. The process is often bilateral | 3-5 days of illness. The process is two-way | 1st day - one-way process |
| Hyperemia of the mucous membrane of the tonsils | Stagnant-cyanotic | Bright | Significant | Absent |
| A sore throat | Moderate, from the first hours of illness increases during the day | Significant, appears by the end of 1 day | Significant | No or moderate |
| Swelling of the tonsils | Moderate | Moderate | Significant | Moderate swelling of one of the tonsils |
| Plaque (overlay) on the palatine tonsils | Forms in the first hours of illness, by the end of the 1st day, filmy, protrudes above the surface of the tissue, after removal the mucous membrane bleeds | The deposits are purulent (follicular, lacunar), and do not protrude above the surface of the tissue. Easy to remove | The deposits protrude above the surface of the tissues, are loose, never extend beyond the tonsils, and may be diphtheritic in nature | The overlays are loose, purulent, located on the surface of the ulcer; when removed, a bleeding defect is exposed |
| Soreness of the affected lymph nodes | Moderate | Significant | Significant | Minor |
| Change in hemogram | Slight neutrophilic leukocytosis | Neutrophilic leukocytosis, a sharp shift in the leukocyte formula to the left | Leukocytosis, lymphocytosis, increased number of mononuclear cells, atypical mononuclear cells | Mild neutrophilic leukocytosis |
| Clinical signs | Differentiable diseases | |||
| oropharyngeal diphtheria toxic form | peritonsillar abscess | parotitis | necrotizing tonsillitis in acute leukemia | |
| Development | Sharp, stormy. High body temperature, up to 40 0 C, chills, headache, fatigue, nausea | Acute, may be gradual, body temperature is high, lasts until the abscess opens | It can be acute or gradual. Body temperature may be normal | Acute, high body temperature |
| A sore throat | Severe, from the first hours of illness, increases during the day | Trismus of the masticatory muscles is pronounced. Improvement after opening the abscess | Often occurs during chewing with irradiation into the ear | Moderate |
| Hyperemia. Swelling of the mucous membrane and cervical tissue | Congestive hyperemia. Swelling of the tonsils appears on the 1st day, unilateral or bilateral, diffuse in nature. Swelling of the cervical tissue from the 2nd day of illness | Swelling of the mucous membrane is one-sided, local bulging, fluctuation, no swelling of the cervical tissue | Swelling of the neck, doughy consistency, painless | Mild hyperemia, slight swelling of the pharyngeal mucosa |
| Raid | Formed from the first hours of illness. Gray, dense, adherent to underlying tissues, mucous membrane bleeds when plaque is removed | Characterized by the presence of plaque and swelling of the soft palate on the same side | No | No |
| Reaction of lymph nodes upon palpation | Severe pain | Sharp pain | Painful | Painful |
| Other Features | In the blood leukocytosis, band shift | History of repeated sore throats, chronic tonsillitis | Other organs may be involved in the process (pancreatitis, meningitis, orchitis) | In the terminal stage, the number of leukocytes decreases, profuse bleeding, hemorrhages on the skin and mucous membranes are possible |
Medical tourism
Medical tourism
Get advice on medical tourism
TREATMENT TACTICS AT THE OUTPATIENT LEVEL:
Diphtheria is not treated on an outpatient basis;
· provision of assistance for emergency indications depending on the prevailing syndrome of the disease, followed by transportation and hospitalization of the patient to an infectious diseases hospital.
Non-drug treatment: No.
Drug treatment: No.
Surgery: No.
Further management:
Monitoring of the patient's condition is carried out by KIZ doctors/general practitioners through medical examination.
Dispensary observation of convalescents:
· convalescents of diphtheria and carriers of toxigenic corynebacteria diphtheria are subject to observation for 3 months after discharge from the hospital;
· the initial examination of the convalescent is carried out by a local doctor or a CIZ doctor together with an otolaryngologist and a cardio-rheumatologist. A monthly examination and bacteriological examination for diphtheria, urine and blood tests, electrocardiography 7-10 days after discharge from the hospital, identification and treatment of diseases of the oropharynx and nose are carried out;
· dispensary observation of carriers of toxigenic corynebacteria diphtheria includes a monthly examination by a local doctor, a clinical health specialist, a bacteriological examination and an examination by an otolaryngologist in order to identify and treat chronic pathologies of the oropharynx and nose;
· deregistration of convalescent diphtheria is carried out no earlier than 3 months after discharge from the hospital, if there are 2 negative tests for diphtheria.
Treatment is not carried out on an outpatient basis.
Criteria for the effectiveness of dispensary observation and treatment of persons who have had diphtheria:
· cessation of excretion of the pathogen;
· restoration of dysfunctions of various organs and systems of the body.
TREATMENT TACTICS AT THE INPATIENT LEVEL: all identified patients with diphtheria, with suspected diphtheria, and carriers of the toxigenic diphtheria pathogen receive treatment in a hospital setting.
Non-drug treatment:
· Mode: in the acute period of the disease and at a later stage, if there are signs of damage to the heart and nervous system, bed rest is indicated.
· Diet: table No. 10, depending on the patient’s condition, tube or parenteral nutrition is used.
Drug treatment:
Etiotropic therapy.
The main treatment is PDS, which neutralizes the diphtheria toxin circulating in the blood (effective only in the early stages of the disease). The dose of serum and route of administration depend on the form of diphtheria and the severity of the disease.
Treatment of diphtheria PDS:
| Form of diphtheria | First dose, thousand IU | Course of treatment, thousand IU |
| Localized diphtheria of the oropharynx: | ||
| Island | 10-15 | 10-20 |
| Membranous | 15-40 | 30-50 |
| Common oropharyngeal diphtheria | 30-50 | 50-70 |
| Subtoxic diphtheria of the oropharynx | 40-60 | 60-100 |
| Toxic diphtheria of the oropharynx: | ||
| I degree | 60-80 | 100-180 |
| II degree | 80-100 | 150-220 |
| III degree | 100-150 | 220-350 |
| Hypertoxic diphtheria of the oropharynx | 150-200 | 350-450 |
| Localized diphtheria of the nasopharynx | 15-20 | 20-40 |
| Localized croup | 15-20 | 30-40 |
| Common croup | 30-40 | 60-80 (up to 100) |
| Localized nasal diphtheria | 10-15 | 20-30 |
Pathogenetic therapy: nonspecific detoxification of the body by intravenous administration of colloid and crystalloid solutions (10% dextrose solution, 0.9% sodium chloride solution).
Symptomatic therapy includes:
antipyretic:
Acetaminophen 500 mg;
Diclofenac sodium 75-150 mg/day
List of essential medicines:
· Purified concentrated anti-diphtheria horse serum (diphtheria toxoid), solution for intramuscular and subcutaneous administration - 10,000 IU in ampoules;
Dextrose 5% - 100, 200, 400 ml
· Sodium chloride solution 0.9% - 100, 200, 400 ml.
List of additional medicines:
· Erythromycin - enteric film-coated tablets 0.2; 0.25 g;
· Clarithromycin - film-coated tablets, 0.25 g, 0.5 g;
Chlorhexidine - solution for local and external use
Acetaminophen tablets 500 mg
· Diclofenac sodium film-coated tablets 25 mg, 50 mg, 100 mg.
Drug comparison table:
| Class | INN | Advantages | Flaws | UD |
| J06 Immune sera and immunoglobulins | Purified concentrated anti-diphtheria serum (diphtheria toxoid) | Is the drug of choice | Rarely - allergic reactions | A |
| J01FA Macrolides | Erythromycin | Active against gram-positive and gram-negative microorganisms | Dyspeptic symptoms, with long-term use liver disorders | IN |
| J01FA Macrolides | Clarithromycin | Active against gram-positive, anaerobic bacteria | Dyspeptic symptoms, allergic reactions | IN |
Indicators of treatment effectiveness:
· persistent normalization of temperature for 3 days or more;
· no intoxication;
· absence of inflammatory process in the oropharynx and/or other localization;
· absence of swelling of the subcutaneous tissue;
· relief of damage to the nervous, cardiac systems, kidneys;
· double negative bacteriological cultures for toxigenic corynebacterium diphtheria from the oropharynx and/or other localizations with an interval of 1-2 days not earlier than the 3rd day of antibiotic withdrawal.
INDICATIONS FOR HOSPITALIZATION, INDICATING THE TYPE OF HOSPITALIZATION
Indications for planned hospitalization: No.
Indications for emergency hospitalization: All identified patients with diphtheria, with suspected diphtheria, and carriers of the toxigenic causative agent of diphtheria are subject to mandatory hospitalization.
ORGANIZATIONAL ASPECTS OF THE PROTOCOL
List of protocol developers with qualification information:
1) Kosherova Bakhyt Nurgalievna - Doctor of Medical Sciences, Professor, RSE at Karaganda State Medical University, Vice-Rector for Clinical Work and Continuing Professional Development, Chief Freelance Infectious Diseasesist of the Ministry of Health of the Republic of Kazakhstan.
2) Abuova Gulzhan Narkenovna - Candidate of Medical Sciences, RSE at the South Kazakhstan State Pharmaceutical Academy, acting. professor, head of the department of infectious diseases and dermatovenerology.
3) Nurpeisova Aiman Zhenaevna - chief freelance infectious disease specialist in the Kostanay region, head of the hepatology center, infectious disease doctor at the KGP “Polyclinic No. 1” of the Health Administration of the Kostanay region.
4) Ekaterina Aleksandrovna Yukhnevich - RSE at the Karaganda State Medical University, clinical pharmacologist.
Disclosure of no conflict of interest: absent.
List of reviewers:
1) Kulzhanova Sholpan Adlgazievna - Doctor of Medical Sciences, Professor, RSE at the Astana Medical University, Head of the Department of Infectious Diseases.
Review conditions: review of the protocol 5 years after its publication and from the date of its entry into force or if new methods with a level of evidence are available.
Mobile application "Doctor.kz"

The free mobile application "Doctor.kz" will help you find: where the right doctor sees you, where to get examined, where to get tested, where to buy medications. The most complete database of clinics, specialists and pharmacies in all cities of Kazakhstan.

The meaning of life is related to the question “What to live for”, and not to the question of how to maintain life. A person's attitude is...

A mushroom is a living organism that forms a separate kingdom of the same name. For a long time they were classified as part of the plant kingdom. But in...

For lovers of “quiet” hunting, mushroom season begins in early summer and lasts until late autumn. And rarely do they...
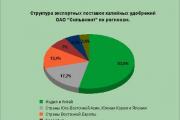
Aleshnikova, V.I. Use of professional consultants. - M.: Infra-M, 1999. - 240 p. 2. Beich, E....

Orange juice. The symbolic meaning of orange juice in dream books is pleasure and temptation. Quite often we...

We most often overcome all kinds of difficulties encountered along the path of life. Of course, for this we make...

This year your patron Neptune will be in your constellation and this is a good sign, because you will...

1993 who? 1993 is the year of which animal? — According to the Chinese horoscope, 1873, 1933, 1993 belonged to the years of the Black...

Wave-particle duality of light means that light simultaneously has the properties of continuous...

The role of biology is enormous in our world. Although it is not one of the priority subjects, most schoolchildren and...

Amines are organic derivatives of ammonia containing an NH 2 amino group and an organic radical. In general...

How to answer questions in Part BThe second part of the social studies work consists of 7 tasks with a short answer....

Form TORG-15 is drawn up in the case when during transportation, movement between and within the warehouse, when...

Nutritionists say that for good health and a slim figure, you must include snacks in your...

A mushroom is a living organism that forms a separate kingdom of the same name. For a long time they were classified as a kingdom...

For lovers of “quiet” hunting, mushroom season begins in early summer and lasts until late autumn. And rarely do they...