Philosophical vision of the problem
The meaning of life is related to the question “What to live for”, and not to the question of how to maintain life. A person's attitude is...
The hand, together with the fingers, ensures the functional and labor activity of a person. Hands, through fine motor skills and finger movements, are involved in understanding the world around us and maintaining a relationship with it. The metacarpophalangeal joint (MCP) connects the phalanges of each finger to the stationary part of the hand. The metatarsophalangeal joints of the legs play a slightly different role. To better understand the structure of the joints, you need to delve into your knowledge of anatomy.
[Hide]
The anatomical structure of the hand includes small bones connected by joints. The hand itself is divided into three zones: the wrist, the metacarpal part and the phalanges of the fingers.
The wrist consists of 8 bones arranged in two rows. The three ossicles of the first row, which have fixed articulations, and the pisiform ossicle adjacent to them, form a common surface and are connected to the radius ossicle. The second row contains four bones connected to the metacarpus. This part is like a boat, with a hollow in the palm. The interosseous space contains nerves, blood vessels along with connective tissue and articular cartilage. The mobility of the bones relative to each other is limited.
The articular part that connects the radius to the wrist allows for rotation and movement. The metacarpal part is formed with 5 bones of a tubular structure. In the proximal part they are attached to the wrist through immovable joints. The opposite side, called the distal side, is connected to the proximal phalanges by movable joints. Due to the spherical metacarpophalangeal joints, flexion and extension of the fingers and rotation of them occur.
The joint of the thumb is saddle-shaped, which allows it only to bend and extend. In the structure of the fingers of the hand, in addition to the thumb, there are three phalanges: the main (proximal), middle and distal (ungual). They are connected by block-shaped interphalangeal movable joints, allowing flexion and extension movements. The thumb is two-phalanx, the middle phalanx is missing.
All carpal joints have strong articular capsules. One capsule is capable of connecting 2-3 joints. The ligamentous structure serves to support the osteoarticular skeleton.
The MCPs of the hands serve as a kind of separator between the fingers and the hand. They protrude from the outside when the hand is bent into a fist. The joint is the base of each of the 5 fingers and provides functional mobility.
The four fingers of the hand act mostly synchronously, with the first finger having a separate function. The second or index finger, due to greater dexterity and independence of movements, grasps an object earlier. The middle finger differs from the others in length and massiveness. Necessary for long-term grip retention. The ring finger is endowed with a developed muscular sense and touch, and the little finger completes the grip and provides stability to the hand when moving.
The design of the joint ensures mobility around the frontal and sagittal axis. Flexion and extension, abduction and adduction movements, and circular movements occur around these axes. Flexion and extension are performed at 90-100 degrees, and adduction and abduction are possible at 45-50 only with extended fingers.
The metacarpophalangeal joints are the articulations of the heads of the metacarpal bones and the sockets of the bases of the proximal phalanges of the fingers. The joints are saddle or condylar. The head of the metacarpal bone is biconvex, and the base itself is biconcave and much smaller in area.
High mobility is explained by the significant difference in size between the articular heads and fossae. They can actively move towards the palm, bend and extend with high amplitude. The function of sweeping lateral movements, that is, abduction and return, is less pronounced. The muscle-tendon system allows them to be converted into rotational movements. The second finger is endowed with the greatest ability for lateral displacement and is called the index finger.
If the articular surfaces were similar, the possibility of displacement would be significantly reduced, which would significantly limit the motor capabilities of the hand.

The interphalangeal joints and MCP joints are characterized by a loose and thin capsule. It is fixed by the solid ligament of the palm and the transverse metacarpal ligaments. On the lateral sides there are collateral ligaments that strengthen the metacarpophalangeal joints and prevent lateral displacement of the finger during flexion. Collateral ligaments originate in the fossae of the ulnar and radial part of the articular surface of the metacarpal bones and the opposite part. Associated with the lateral and palmar portion of the proximal phalanx.
The two ligaments of the flexor and extensor retinaculum on the back of the hand form fibrous sheaths for the muscles. Fibrous sheaths and synovial spaces protect the tendons from injury.
Accessory ligaments are located in the palmar part of the capsule and are called palmar. The fibers of the ligament are woven with the transverse metacarpal ligament between the apices of the II-V bones and keep the apices of the metacarpal bones from moving in different directions.
The intertendinous tissues help retain the extensor muscle. They connect the tendons of pairs of fingers: index and middle, middle and ring, little and ring fingers. Located close to the PFJ. The main tendon near the extensor muscle is divided into superficial, located in the center, and deep, located on the sides.

The articular membrane is covered by the tendon of the flexor muscle on the back side and the tendons of the lumbrical and interosseous muscles. The fibers of these muscles support the flexor muscle due to its location above its tendons. Sagittal bundles are called retinaculum fibers. They are divided into radial or medial, and ulnar or lateral.
The tissues of the bundles are located in a thin layer on the surface and denser in depth. The superficial layer entwines the flexor tendons from above and connects to the sagittal fascicle on the opposite side. Deeper under the tendon, a depression is formed in the form of a channel, stabilizing and maintaining the tendon in one place.
The muscles that allow you to bend and extend your fingers run along the back of the forearm. Their tendon fibers extend throughout the hand to the tips of the MCP joint. They are attached to the middle and tops of the fingers. The extreme fingers, the little finger and the index finger, have additional extensor muscles. The tendons of these muscles are located at the upper points of the corresponding MCP joint along with the common digital extensor and are balanced by similar structures.

The mobility of the hand joints allows you to grasp and hold various objects. The fulfillment of this task is ensured by the mobility of the thumb, which is opposed to the rest.
The MTP joint of the thumb, although externally similar to the others, has differences in structure. First of all, the trochlear joint is different. It is saddle-shaped and its articular head is much larger, the tubercles on the palmar side are more developed. Articular capsule, on the surface facing the palm, with two sesamoid bones: lateral and medial. The part facing the cavity is covered by hyaline cartilage, and the long flexor tendon passes between the bones.
The shape of the articular surfaces ensures finger mobility in two planes: extension and flexion, abduction and reverse movement. The effectiveness of the palm grip is ensured by the special structure of the ligaments and tendons on the hand, in which the flexion of the index finger and little finger is directed towards the thumb.

The distal part of the lower limb is the foot, which is necessary to hold the body in an upright position. Its structure is a complex combination of groups of small bones that form a strong arch to support the body when moving and in a standing position. This design and the large number of joints create a flexible and durable structure. The lower arch of the foot in contact with the ground is called the sole, the opposite part is called the back.
The skeleton of the human foot includes 26 bones, divided into three parts: the tarsus, metatarsus and the phalanges of the toes.

The interphalangeal joints of the toe joints are called the metatarsophalangeal, proximal and distal joints. The structure of the first toe is similar to the big toe. It has only two phalanges, while the rest of the fingers have three. The mobility of the joints of the foot is similar to the corresponding carpal joints, but with restrictions. The toes are slightly retracted to the sides and back, have developed dorsal flexion and slightly less developed plantar flexion. Their extension is greater than flexion.
At the site of the ligament of the heads of the metatarsal bones with the lower part of the proximal phalanges there is a metatarsophalangeal ball-and-socket joint. On the back side, the joints of the toes are closed by extensors, and on the sole by tendon channels. On both sides the joints are strengthened by lateral ligaments. From the side of the sole – intercapitate ligaments and tendons.
The joint of the first finger is strengthened on the inside by the tendon of the abductor muscle. On the outer side it is adjacent to the tissue of the interdigital space. In the plantar part, the capsule includes the internal and external sesamoid ossicles.
The metatarsophalangeal joint of the second toe on the plant side is strengthened by the fibers of the fibrous canal of the flexor muscles. The tendon fibers of the intercapitate ligament and adductor muscle are woven into the capsule. On the inside it is supported by a ligament of tendons of the first dorsalis muscle, and under the ligament by the tendons of the lumbrical muscle.
The capsule is strengthened from the outside by the tendons of the dorsal interosseous muscle. On both sides of the capsule there is fiber in the interdigital spaces. The heads of all metatarsal bones are braided by a deep transverse ligament. The flexion angle of the metatarsophalangeal joints is small, which is associated with the high density of the joint capsule.
Why joint deformation occurs and what it looks like, as well as how to carry out treatment, watch the video.
Based on an analysis of 2147 cases of closed fractures E. V. Usoltseva found that multiple ones occur in 29.3% of cases. Fractures of the fingers of the left hand are more common than those of the right hand. Injuries to the index finger account for 30% and are the most common. This is followed by the middle finger (22.9%), then the thumb (19.1%), little finger (18.3%) and finally the ring finger (13.7%).
Incidence of terminal phalanx fractures 47%, primary - 31.2%, intermediate - 8.6%, and the incidence of metacarpal bone fractures is 13.2%. Types of hand bone fractures are shown in the figure.
Rules treatment of hand fractures the same as for any other fractures, that is, repositioning, immobilization and functional therapy. The thin structure of the hand reacts very unfavorably to changes associated with injuries and immobilization, as well as to residual bone deformities. Shortening, twisting, and displacement that remain after healing of fractures disrupt not only the function of the injured finger, but the entire hand as a whole.
At repositions And hand immobilization It should be taken into account that only the middle finger moves in accordance with the axis of the hand, and the remaining fingers, when bent, are directed towards the scaphoid bone.
Necessary accept Keep in mind that the ability of hand bones to regenerate varies and depends on the location of the fracture. Epiphyses of a spongy structure grow together faster (3-5 weeks) than poorly vascularized diaphyses of a cortical structure (10-14 weeks). Moberg's diagram shows the time of immobilization required for fusion of fragments (The long period of fusion of the diaphysis of the second phalanx is especially striking.

For prolonged immobilization a necessary condition is to fix the limb in a functionally advantageous position and create the opportunity for movements of the intact parts of the hand. Otherwise, the functional condition of the hand deteriorates during treatment.
Fractures of the terminal phalanges usually heal without complications. If there is a fracture of the area (the ralang on which the nail is located), then for immobilization an aluminum or plaster splint should be applied to the palmar surface of the two distal phalanges. These fractures are often accompanied by a subungual hematoma, which is extremely painful and easily suppurates. Therefore, the hematoma should be removed by drilling the nail or raising a small area of it.Trephination should be carried out under aseptic conditions.
Nail process, as a rule, undergoes fractures due to open injuries. It, together with the nail and part of the flesh of the finger, dislocates towards the palm. Reposition of the bone, nail and flesh of the finger is performed simultaneously. The nail is fixed with one or two sutures - this is the best splinting for the broken part of the phalanx.
Splintered body fractures and the bases of the terminal phalanx are often fixed with a thin bone Kirschner wire, without splinting, since only in this way sufficient fixation of the broken bone and the shortest period of immobilization are ensured.
 With rotational displacement, the lines of the nail plates are not parallel compared to the nail plates of the fingers of the uninjured hand
With rotational displacement, the lines of the nail plates are not parallel compared to the nail plates of the fingers of the uninjured hand
On medium and basic phalanges differ: cracks, epiphysiolysis and complete fractures.
Fracture location May be:
a) on the head,
b) on the diaphysis and
c) based on.
 Aluminum splint (1), used in the treatment of fractures of the main phalanx using the conservative method according to Iselen; the splint is previously modeled according to the corresponding finger of a healthy hand.
Aluminum splint (1), used in the treatment of fractures of the main phalanx using the conservative method according to Iselen; the splint is previously modeled according to the corresponding finger of a healthy hand. A) Head fractures may have a transverse “Y” or “V” shape. An intra-articular fracture of one or both condyles usually simulates a dislocation. In the presence of comminuted fractures, resection followed by arthroplasty may be necessary.
b) The fracture line of the diaphysis can be transverse, oblique, oblong and multiple. When the middle phalanx is fractured, due to the displacement of the fragments, an angle is formed that is open to the rear and very rarely to the palmar side (if the fracture line is localized proximal to the attachment of the superficial flexor tendon). When the main phalanx is fractured, an angle is formed that is also open to the rear, since the dorsal aponeurosis, due to the action of the common extensor digitorum of the lumbrical and interosseous muscles, becomes tense.
Reduction of diaphyseal fractures is not difficult, however, maintaining the fragments in the reduced position is not easy, especially in the presence of transverse fractures.
V) Fractures of the base of the middle and main phalanges may have a transverse "Y" or "V" shape, or may be jagged.
At treatment of fractures of the middle and main phalanges It should be remembered that satisfactory fixation of the fingers cannot be achieved without immobilization of the wrist joint. To do this, a fingerless plaster glove is placed on the hand, including the radiocarpal joint, providing a functionally advantageous position. A palmar curved wire splint is attached to the plaster glove distal to the main phalanx for the broken finger or fingers. After reposition, the finger is fixed on the splint using an adhesive patch. If this is not sufficient, then you should resort to adhesive traction.
Traction should not last more than three weeks. After removing it, only a protective splint is applied to prevent the fragments from moving. With the Bunnell method, transmuscular traction is used, and according to Moberg, transosseous traction is used. We consider these two methods to be incorrect. The traction with a rubber band is difficult to regulate, sometimes it is too strong, and in other cases it is easily weakened. This method requires constant x-ray monitoring. The method is dangerous due to the possibility of infection and skin necrosis. The traction exerted on the finger during traction treatment does not serve to reposition the fragments, but only to fix the manually reduced bones.
 a - diagram of the displacement of fragments occurring during fractures of the middle phalanx
a - diagram of the displacement of fragments occurring during fractures of the middle phalanx If fixation is not achieved by applying an adhesive bandage or traction, then we resort to the method of trans- or intraosseous fixation using Kirschner wires, but in no case do we consider the use of excessive traction acceptable. Transosseous wire fixation has its advantages even in the presence of open fractures. We combined it with the introduction of antibiotics, as a result of which we never observed infectious complications. Verdun suggests the use of periosteal fixation using a pin. After manual reduction, a thin Kirschner wire is inserted between the extensor tendon and the cortical bone, which prevents the fragments from moving at an angle or to the side.
According to our personal experience, in the presence of transverse fractures, such an “internal” splint is not sufficient, since it does not prevent the rotation of the distal fragment of the phalanx. To immobilize such fractures, cross-wires should be used (I. Böhler, Strehli).
The human hand has a complex structure and performs a variety of subtle movements. It is a working organ and, as a result, is more often damaged than other parts of the body.
Introduction.
The structure of injuries is dominated by industrial (63.2%), household (35%) and street (1.8%) types of injuries. Industrial injuries are usually open and account for 78% of all open injuries of the upper extremities. Damage to the right hand and fingers is 49%, and to the left – 51%. Open injuries of the hand in 16.3% of cases are accompanied by combined damage to tendons and nerves due to their close anatomical location. Injuries and diseases of the hand and fingers lead to disruption of their function, temporary loss of ability to work, and often to disability of the victim. The consequences of injuries to the hand and fingers account for more than 30% of the disability structure due to damage to the musculoskeletal system. The loss of one or more fingers leads to professional and psychological difficulties. The high percentage of disability as a result of injuries to the hand and fingers is explained not only by the severity of the injuries, but also by incorrect or untimely diagnosis and choice of treatment tactics. When treating this group of patients, one should strive to restore not only the anatomical integrity of the organ, but also its function. Surgical treatment of injuries is carried out according to an individual plan and in accordance with the principles outlined below.
Features of treatment of patients with injuries and diseases of the hand.
Anesthesia.
The main condition for performing fine intervention on the hand is adequate pain relief. Local infiltration anesthesia can only be used for superficial defects; its use is limited on the palmar surface of the hand due to low skin mobility.
In most cases, during hand surgeries, conduction anesthesia is performed. Blocking the main nerve trunks of the hand can be carried out at the level of the wrist, elbow joint, axillary and cervical region. For finger surgery, anesthesia according to Oberst-Lukashevich or a block at the level of the intermetacarpal spaces is sufficient (see Fig. 1)
Fig. 1 Points of injection of anesthetic during conduction anesthesia of the upper limb.
At the level of the fingers and wrist, it is necessary to avoid the use of prolonged anesthetics (lidocaine, marcaine), since, due to prolonged resorption of the drug, compression of the neurovascular bundles and the occurrence of tunnel syndromes, and in some cases, necrosis of the finger, may occur. For severe hand injuries, anesthesia should be used.
Bleeding of the surgical field.
Among blood-soaked tissues, it is impossible to differentiate the vessels, nerves and tendons of the hand, and the use of tampons to remove blood from the surgical field causes harm to the gliding apparatus. Therefore, bleeding is mandatory not only for major interventions on the hand, but also when treating minor injuries. To bleed the hand, an elastic rubber bandage or a pneumatic cuff is applied to the upper third of the forearm or lower third of the shoulder, in which pressure is injected to 280-300 mm Hg, which is more preferable, as it reduces the risk of nerve paralysis. Before using them, it is advisable to apply an elastic rubber bandage to a previously raised arm, which helps to force out a significant part of the blood from the arm. To operate on a finger, it is enough to apply a rubber tourniquet at its base. If the surgical intervention lasts more than 1 hour, then it is necessary to release the air from the cuff for a few minutes with the limb elevated, and then fill it again.
Skin incisions on the hand.
The epidermis on the hand forms a complex network of lines, the direction of which is determined by various movements of the fingers. On the palmar surface of the skin of the hand there are many furrows, wrinkles and folds, the number of which is not constant. Some of them, which have a specific function and are landmarks of deeper anatomical formations, are called primary skin formations (Fig. 2).

Fig. 2 Primary skin formations of the hand.
1-distal palmar groove, 2-proximal palmar groove. 3-interphalangeal grooves, 4-palmar carpal grooves, 5-interdigital folds, 6-interphalangeal folds
From the base of the main grooves, connective tissue bundles extend vertically to the palmar aponeurosis and to the tendon sheaths. These grooves are the “joints” of the skin of the hand. The groove plays the role of an articular axis, and adjacent areas perform movements around this axis: approaching each other - flexion, moving away - extension. Wrinkles and folds are reservoirs of movement and contribute to an increase in skin surface.
A rational skin incision should be subject to minimal stretching during movement. Due to constant stretching of the edges of the wound, hyperplasia of the connective tissue occurs, the formation of rough scars, their wrinkling and, as a result, dermatogenous contracture. Incisions perpendicular to the grooves undergo the greatest change with movement, while incisions parallel to the grooves heal with minimal scarring. There are areas of the hand skin that are neutral in terms of stretching. Such an area is the midlateral line (Fig. 3), along which stretching in opposite directions is neutralized.

Fig. 3 Medial lateral line of the finger.
Thus, the optimal incisions on the hand are those parallel to the primary skin formations. If it is impossible to provide such access to damaged structures, it is necessary to select the most correct permissible type of incision (Fig. 4):
1. the incision parallel to the furrows is complemented by a straight or arcuate one of the wrong direction,
2. the incision is made along the neutral line,
3. an incision perpendicular to the grooves is complemented by a Z-shaped plastic,
4. The incision crossing the primary skin formations should be arcuate or Z-shaped to redistribute tensile forces.

Rice. 4A-Optimal cuts on the hand,B-Z-plastic
For optimal primary surgical treatment of hand injuries, it is necessary to widen the wounds through additional and lengthening incisions in the correct direction. (Fig. 5)

Fig. 5 Additional and lengthening incisions on the hand.
Atraumatic surgical technique.
Hand surgery is surgery of sliding surfaces. The surgeon must be aware of two dangers: infection and trauma, which ultimately lead to fibrosis. To avoid it, a special technique is used, which Bunnel called atraumatic. To implement this technique, it is necessary to observe the strictest asepsis, use only sharp instruments and thin suture material, and constantly moisturize the tissue. Trauma to tissues with tweezers and clamps should be avoided, since micronecrosis forms at the site of compression, leading to scarring, as well as leaving foreign bodies in the wound in the form of long ends of ligatures and large nodes. It is important to avoid the use of dry swabs to stop bleeding and tissue preparation, and also to avoid unnecessary wound drainage. The skin edges should be joined with minimal tension and without interfering with the blood supply to the flap. The so-called “time factor” plays a huge role in the development of infectious complications, since too long operations lead to “fatigue” of tissues and a decrease in their resistance to infection.
After atraumatic intervention, the tissues retain their characteristic luster and structure, and during the healing process only a minimal tissue reaction occurs
Immobilization of the hand and fingers.
The human hand is in constant motion. A stationary state is unnatural for the hand and leads to serious consequences. The idle hand assumes a resting position: slight extension at the wrist joint and flexion at the finger joints, abduction of the thumb. The hand takes a resting position lying on a horizontal surface and hanging (Fig. 6)

Fig.6 Hand in rest position
In the functional position (position of action), extension in the wrist joint is 20, ulnar abduction is 10, flexion in the metacarpophalangeal joints is 45, in the proximal interphalangeal joints - 70, in the distal interphalangeal joints - 30, the first metacarpal bone is in a state of opposition, and the great The finger forms an incomplete letter “O” with the index and middle fingers, and the forearm occupies a position midway between pronation and supination. The advantage of the functional position is that it creates the most favorable starting position for the action of any muscle group. The position of the finger joints depends on the position of the wrist joint. Flexion at the wrist joint causes extension of the fingers, and extension causes flexion (Fig. 7).

Fig.7 Functional position of the hand.
In all cases, in the absence of forced circumstances, it is necessary to immobilize the hand in a functional position. Immobilizing the finger in a straight position is an irreparable mistake and leads to stiffness in the finger joints in a short time. This fact is explained by the special structure of the collateral ligaments. They extend distally and palmarly from the rotation points. Thus, in a straightened position of the finger, the ligaments relax, and in a bent position they become tense (Fig. 8).

Fig. 8 Biomechanics of collateral ligaments.
Therefore, when the finger is fixed in an extended position, the ligament shrinks. If only one finger is damaged, the rest should be left free.
Fractures of the distal phalanx.
Anatomy.
Connective tissue septa, stretching from the bone to the skin, form a cellular structure and participate in stabilizing the fracture and minimizing the displacement of fragments. (Fig. 9)

R Fig.9 Anatomical structure of the nail phalanx:1-attachment of collateral ligaments,2- connective tissue septa,3-lateral interosseous ligament.
On the other hand, a hematoma that occurs in closed connective tissue spaces is the cause of a bursting pain syndrome that accompanies damage to the nail phalanx.
The extensor and deep flexor tendons of the finger, attached to the base of the distal phalanx, do not play a role in the displacement of the fragments.
Classification.
There are three main types of fractures (according to Kaplan L.): longitudinal, transverse and comminuted (eggshell type) (Fig. 10).

Rice. 10 Classification of fractures of the nail phalanx: 1-longitudinal, 2-transverse, 3-comminuted.
Longitudinal fractures in most cases are not accompanied by displacement of fragments. Transverse fractures of the base of the distal phalanx are accompanied by angular displacement. Comminuted fractures involve the distal phalanx and are often associated with soft tissue injuries.
Treatment.
Non-displaced and comminuted fractures are treated conservatively. For immobilization, palmar or dorsal splints are used for a period of 3-4 weeks. When applying a splint, it is necessary to leave the proximal interphalangeal joint free (Fig. 11).

Fig. 11 Splints used to immobilize the nail phalanx
Transverse fractures with angular displacement can be treated both conservatively and surgically - closed reduction and osteosynthesis with a thin Kirschner wire (Fig. 12).

Fig. 12 Osteosynthesis of the nail phalanx with a thin Kirschner wire: A, B - stages of the operation, C - Final type of osteosynthesis.
Fractures of the main and middle phalanges.
The displacement of phalangeal fragments is primarily determined by muscle traction. With unstable fractures of the main phalanx, the fragments are displaced at an angle towards the rear. The proximal fragment assumes a bent position due to the traction of the interosseous muscles attached to the base of the phalanx. The distal fragment does not serve as an attachment point for the tendons and its hyperextension occurs due to the traction of the central portion of the extensor tendon of the finger, which is attached to the base of the middle phalanx (Fig. 13). 
Fig. 13 The mechanism of displacement of fragments in fractures of the main phalanx
In case of fractures of the middle phalanx, it is necessary to take into account two main structures that influence the displacement of fragments: the middle portion of the extensor tendon, attached to the base of the phalanx from the rear, and the superficial flexor tendon, attached to the palmar surface of the phalanx (Fig. 14)

Fig. 14. Mechanism of displacement of fragments in fractures of the middle phalanx
Particular attention should be paid to fractures with rotational displacement, which must be eliminated especially carefully. In a bent position, the fingers are not parallel to each other. The longitudinal axes of the fingers are directed towards the scaphoid bone (Fig. 15)

When the phalanges are fractured with displacement, the fingers intersect, which makes functioning difficult. In patients with phalangeal fractures, flexion of the fingers is often impossible due to pain, so rotational displacement can be determined by the location of the nail plates in a semi-flexed position of the fingers (Fig. 16)

Fig. 16 determination of the direction of the longitudinal axis of the fingers for phalangeal fractures
It is extremely important that the fracture heals without permanent deformation. The sheaths of the flexor tendons pass in the palmar groove of the phalanges of the fingers and any irregularity prevents the tendons from sliding.
Treatment.
Non-displaced or impacted fractures can be treated using so-called dynamic splinting. The damaged finger is fixed to the neighboring one and early active movements begin, which prevents the development of stiffness in the joints. Displaced fractures require closed reduction and fixation with a plaster cast (Fig. 17)

Fig. 17 use of a plaster splint for fractures of the phalanges of the fingers
If after reposition the fracture is not stable, the fragments cannot be held using a splint, then percutaneous fixation with thin Kirschner wires is necessary (Fig. 18)

Fig. 18 Osteosynthesis of the phalanges of the fingers using Kirschner wires
If closed reduction is impossible, open reduction is indicated, followed by osteosynthesis of the phalanx with knitting needles, screws, and plates. (Fig. 19)

Fig. 19 Stages of osteosynthesis of the phalanges of the fingers with screws and a plate
For intra-articular fractures, as well as comminuted fractures, the best treatment result is provided by the use of external fixation devices.
Fractures of the metacarpal bones.
Anatomy.
The metacarpal bones are not located in the same plane, but form the arch of the hand. The arch of the wrist meets the arch of the hand, forming a semicircle, which is completed to a full circle by the first finger. This way the fingertips touch at one point. If the arch of the hand flattens due to damage to bones or muscles, a traumatic flat hand is formed.
Classification.
Depending on the anatomical location of the damage, there are: fractures of the head, neck, diaphysis and base of the metacarpal bone.
Treatment.
Fractures of the metacarpal head require open reduction and fixation with thin Kirschner wires or screws, especially in the case of an intra-articular fracture.
Metacarpal neck fractures are a common injury. The fracture of the neck of the fifth metacarpal bone, as the most common, is called the “boxer’s fracture” or “fighter’s fracture.” Such fractures are characterized by displacement at an angle open to the palm and are unstable due to destruction of the palmar cortical layer (Fig. 20)

Fig. 20 Fracture of the metacarpal neck with destruction of the palmar cortical plate
With conservative treatment by immobilization with a plaster splint, it is usually not possible to eliminate the displacement. The bone deformation does not have a significant effect on the function of the hand; only a small cosmetic defect remains. To effectively eliminate displacement of fragments, closed reduction and osteosynthesis with two intersecting Kirschner wires or transfixation with wires to the adjacent metacarpal bone are used. This method allows you to start early movements and avoid stiffness in the joints of the hand. The wires can be removed 4 weeks after surgery.
Fractures of the diaphysis of the metacarpal bones are accompanied by significant displacement of fragments and are unstable. With direct force, transverse fractures usually occur, and with indirect force, oblique fractures occur. Displacement of fragments leads to the following deformations: formation of an angle open to the palm (Fig. 21)

Fig. 21 The mechanism of displacement of fragments during a fracture of the metacarpal bone.
Shortening of the metacarpal bone, hyperextension in the metacarpophalangeal joint due to the action of the extensor tendons, flexion in the interphalangeal joints caused by displacement of the interosseous muscles, which, due to the shortening of the metacarpal bones, are no longer able to perform the extension function. Conservative treatment in a plaster splint does not always eliminate displacement of fragments. For transverse fractures, transfixation with pins to the adjacent metacarpal bone or intramedullary seosynthesis with a pin is most effective (Fig. 22)

Fig. 22 Types of osteosynthesis of the metacarpal bone: 1- with knitting needles, 2- with plate and screws
For oblique fractures, osteosynthesis is performed using AO miniplates. These methods of osteosynthesis do not require additional immobilization. Active movements of the fingers are possible from the first days after surgery after swelling subsides and pain decreases.
Fractures of the base of the metacarpal bones are stable and do not pose difficulties for treatment. Immobilization with a dorsal splint reaching the level of the heads of the metacarpal bones for three weeks is quite sufficient for healing of the fracture.
Fractures of the first metacarpal bone.
The unique function of the first finger explains its special position. Most fractures of the first metacarpal are base fractures. By Green D.P. These fractures can be divided into 4 types, and only two of them (Bennett’s fracture-dislocation and Rolando’s fracture) are intra-articular (Fig. 23)

Rice. 23 Classification of fractures of the base of the first metacarpal bone: 1 - Bennett fracture, 2 - Rolando fracture, 3,4 - extra-articular fractures of the base of the first metacarpal bone.
To understand the mechanism of injury, it is necessary to consider the anatomy of the first carpometacarpal joint. The first carpometacarpal joint is a saddle joint formed by the base of the first metacarpal bone and the trapezium bone. Four main ligaments are involved in stabilizing the joint: anterior oblique, posterior oblique, intermetacarpal and dorsal radial. (Fig. 24)

Fig. 24 Anatomy of the first metacarpophalangeal joint
The volar portion of the base of the first metacarpal is somewhat elongated and is the site of attachment of the anterior oblique ligament, which is key to the stability of the joint.
For the best visualization of the joint, radiography is required in the so-called “true” anterior-posterior projection (Robert projection), when the hand is in the position of maximum pronation (Fig. 25)

Fig.25 Robert's projection
Treatment.
Bennett's fracture-dislocation results from direct trauma to the subflexed metacarpal. At the same time it happens
dislocation, and a small triangular-shaped volar bone fragment remains in place due to the force of the anterior oblique ligament. The metacarpal bone is displaced to the radial side and to the rear due to the traction of the abductor longus muscle (Fig. 26).
Fig. 26 Bennett's fracture-dislocation mechanism
The most reliable method of treatment is closed reduction and percutaneous fixation with Kirschner wires to the second metacarpal or to the trapezius bone or trapezium bone (Fig. 27)

Fig. 27 Osteosynthesis using Kirschner wires.
For reposition, traction is performed on the finger, abduction and opposition of the first metacarpal bone, at the moment of which pressure is applied to the base of the bone and reposition. In this position, the needles are inserted. After the operation, immobilization is performed in a plaster splint for a period of 4 weeks, after which the splint and wires are removed and rehabilitation begins. If closed reduction is not possible, they resort to open reduction, after which osteosynthesis is possible using both Kirschn wires and thin 2 mm AO screws.
Rolando's fracture is a T- or Y-shaped intra-articular fracture and can be classified as a comminuted fracture. The prognosis for restoration of function with this type of injury is usually unfavorable. In the presence of large fragments, open reduction and osteosynthesis with screws or wires are indicated. To preserve the length of the metacarpal bone, external fixation devices or transfixation to the second metacarpal bone are used in combination with internal fixation. In case of compression of the base of the metacarpal bone, primary bone grafting is necessary. If it is impossible to surgically restore the congruence of the articular surfaces, as well as in elderly patients, a functional method of treatment is indicated: immobilization for a minimum period for pain to subside, and then early active movements.
Extra-articular fractures of the third type are the most rare fractures of the first metacarpal bone. Such fractures respond well to conservative treatment - immobilization in a plaster splint in a hyperextension position in the metacarpophalangeal joint for 4 weeks. Oblique fractures with a long fracture line may be unstable and require percutaneous osteosynthesis with wires. Opening reduction for these fractures is used extremely rarely.
Scaphoid fractures
Scaphoid fractures account for up to 70% of all wrist fractures. They occur when falling on an outstretched hand due to hyperextension. According to Russe, horizontal, transverse and oblique fractures of the scaphoid are distinguished. (fig28)
Recognizing these fractures can be quite difficult. Local pain when pressing on the area of the anatomical snuffbox, pain when dorsiflexing the hand, as well as radiography in a direct projection with some supination and ulnar abduction of the hand are important.
Conservative treatment.
Indicated for fractures without displacement of fragments. Plaster immobilization in a bandage covering the thumb for 3-6 months. The plaster casts are changed every 4-5 weeks. To assess consolidation, it is necessary to conduct staged radiographic studies, and in some cases MRI (Fig. 29).

Fig. 29 1- MRI picture of a scaphoid fracture,2- immobilization for scaphoid fractures
Surgical treatment.
Open reduction and screw fixation.
The scaphoid bone is exposed through access along the palmar surface. Then a guide pin is passed through it through which a screw is inserted. The most commonly used screw is Herbert, Acutrak, AO. After osteosynthesis, plaster immobilization for 7 days (Fig. 30)

Fig. 30 Osteosynthesis of the scaphoid bone with a screw
Nonunion of the scaphoid bone.
For nonunions of the scaphoid bone, bone grafting according to Matti-Russe is used. Using this technique, a groove is formed in the fragments into which cancellous bone taken from the iliac crest or from the distal radius is placed (D.P. Green) (Fig. 31). Plaster immobilization 4-6 months.

Fig. 31 Bone grafting for nonunion of the scaphoid.
Screw fixation with or without bone grafting can also be used.
Damage to small joints of the hand.
Damage to the distal interphalangeal joint.
Dislocations of the nail phalanx are quite rare and usually occur on the dorsal side. More often, dislocations of the nail phalanx are accompanied by avulsion fractures of the attachment sites of the tendons of the deep flexor or extensor of the finger. In fresh cases, open reduction is performed. After reduction, lateral stability and the nail phalanx hyperextension test are checked. If there is no stability, transarticular fixation of the nail phalanx is performed with a pin for a period of 3 weeks, after which the pin is removed. Otherwise, immobilization of the distal interphalangeal joint in a plaster splint or a special splint for 10-12 days is indicated. In cases where more than three weeks have passed since the injury, it is necessary to resort to open reduction, followed by transarticular fixation with a pin.
Injuries to the proximal interphalangeal joint.
The proximal interphalangeal joint occupies a special place among the small joints of the hand. Even if there is no movement in the other joints of the finger, with preserved movements in the proximal interphalangeal joint, hand function remains satisfactory. When treating patients, it is necessary to take into account that the proximal interphalangeal joint is prone to stiffness not only with injuries, but also with prolonged immobilization of even a healthy joint.
Anatomy.
The proximal interphalangeal joints are block-shaped in shape and are strengthened by collateral ligaments and the palmar ligament.
Treatment.
Damage to collateral ligaments.
Injury to the collateral ligaments occurs as a result of the application of lateral force to a straightened toe, most commonly seen during sports. The radial radial ligament is injured more often than the ulnar ligament. Collateral ligament injuries diagnosed 6 weeks after injury should be considered old. It is important to check lateral stability and perform stress radiography to make a diagnosis. When assessing the results of these tests, it is necessary to focus on the amount of lateral movement of healthy fingers. To treat this type of injury, the method of elastic splinting is used: the injured finger is fixed to the adjacent one for 3 weeks in case of partial ligament rupture and for 4-6 weeks in case of complete rupture, then sparing of the finger is recommended for another 3 weeks (for example, avoiding sports activities). (Fig. 32)
Fig. 32 Elastic splinting for injuries of collateral ligaments
During the period of immobilization, active movements in the joints of the injured finger are not only not contraindicated, but are absolutely necessary. In the treatment of this group of patients, it is necessary to take into account the following facts: full range of motion is restored in the vast majority of cases, while pain persists for many months, and the increase in joint volume in some patients lasts a lifetime.
Dislocations of the middle phalanx.
There are three main types of dislocations of the middle phalanx: dorsal, palmar and rotational (rotatory). For diagnosis, it is important to take x-rays of each damaged finger separately in direct and strictly lateral projections, since oblique projections are less informative (Fig. 33)
Fig. 33 X-ray for dorsal dislocations of the middle phalanx.
The most common type of injury is dorsal dislocation. It is easy to eliminate, often done by the patients themselves. Elastic splinting for 3-6 weeks is sufficient for treatment.
With a palmar dislocation, damage to the central portion of the extensor tendon is possible, which can lead to the formation of a “boutonniere” deformity (Fig. 34)
Fig. 34 Boutonniere finger deformity
To prevent this complication, a dorsal splint is used that fixes only the proximal interphalangeal joint for 6 weeks. During the period of immobilization, passive movements are performed in the distal interphalangeal joint (Fig. 35)

Fig. 35 Prevention of boutonniere-type deformation
Rotational subluxation is easily confused with palmar subluxation. On a strictly lateral radiograph of the finger, you can see the lateral projection of only one of the phalanges and the oblique projection of the other (Fig. 36)
Fig. 36 Rotational dislocation of the middle phalanx.
The reason for this damage is that the condyle of the head of the main phalanx falls into a loop formed by the central and lateral portions of the extensor tendon, which is intact (Fig. 37).

Fig. 37 rotational dislocation mechanism
Reduction is carried out according to the Eaton method: after anesthesia, the finger is flexed at the metacarpophalangeal and proximal interphalangeal joint, and then carefully rotated the main phalanx (Fig. 38)

Fig. 38 Reduction of rotatory dislocation according to Eaton
In most cases, closed reduction is not effective and it is necessary to resort to open reduction. After reduction, elastic splinting and early active movements are performed.
Fractures and dislocations of the middle phalanx.
As a rule, a fracture of the palmar fragment of the articular surface occurs. This joint-destructive injury can be successfully treated if diagnosed early. The simplest, non-invasive and effective method of treatment is the use of a dorsal extension locking splint (Fig. 39), applied after reduction of the dislocation and allowing active flexion of the finger. Full reduction requires flexion of the finger at the proximal interphalangeal joint. Reduction is assessed using a lateral radiograph: the adequacy of reduction is assessed by the congruence of the intact dorsal part of the articular surface of the middle phalanx and the head of the proximal phalanx. The so-called V-sign, proposed by Terri Light, helps in assessing the radiograph (Fig. 40)

Fig. 39 Dorsal extension blocking splint.
Fig.40 V-sign for assessing the congruence of the articular surface.
The splint is applied for 4 weeks, and is extended weekly by 10-15 degrees.
Damage to the metacarpophalangeal joints.
Anatomy.
Metacarpophalangeal joints are condylar joints that allow, along with flexion and extension, adduction, abduction and circular movements. The stability of the joint is provided by the collateral ligaments and the palmar plate, which together form a box shape (Fig. 41)

Fig. 41 Ligamentous apparatus of the metacarpophalangeal joints
Collateral ligaments consist of two bundles - proper and accessory. The collateral ligaments are more tense during flexion than during extension. The palmar plates of fingers 2-5 are connected to each other by the deep transverse metacarpal ligament
Treatment.
There are two types of finger dislocation: simple and complex (irreducible). For the differential diagnosis of dislocations, it is necessary to remember the following signs of a complex dislocation: on the radiograph, the axis of the main phalanx and metacarpal bone are parallel, the sesamoid bones may be located in the joint, and there is a depression of the skin on the palmar surface of the hand at the base of the finger. A simple dislocation can be easily corrected by applying gentle pressure to the main phalanx without requiring traction. Elimination of a complex dislocation is possible only surgically.
Damage to the nail bed.
The nail gives the distal phalanx hardness when gripping, protects the fingertip from injury, plays an important role in the function of touch and in the perception of the aesthetic appearance of a person. Injuries to the nail bed are among the most common injuries of the hand and accompany open fractures of the distal phalanx and injuries to the soft tissues of the fingers.
Anatomy.
The nail bed is the layer of dermis that lies beneath the nail plate.

Rice. 42 Anatomical structure of the nail bed
There are three main zones of tissue located around the nail plate. The nail fold (roof of the matrix), covered with an epithelial lining - eponychium, prevents uncontrolled growth of the nail upwards and to the sides, directing it distally. In the proximal third of the nail bed there is the so-called germinal matrix, which ensures nail growth. The growing part of the nail is delimited by a white crescent - a hole. If this area is damaged, the growth and shape of the nail plate are significantly disrupted. Distal to the socket is a sterile matrix that fits tightly to the periosteum of the distal phalanx, allowing the advancement of the nail plate as it grows and thus playing a role in the formation of the shape and size of the nail. Damage to the sterile matrix is accompanied by deformation of the nail plate.
The nail grows at an average rate of 3-4 mm per month. After injury, distal advancement of the nail stops for 3 weeks, and then nail growth continues at the same rate. As a result of the delay, a thickening forms proximal to the injury site, persisting for 2 months and gradually becoming thinner. It takes about 4 months before a normal nail plate forms after an injury.
Treatment.
The most common injury is a subungual hematoma, which is clinically manifested by the accumulation of blood under the nail plate and is often accompanied by severe pain of a pulsating nature. The treatment method is to perforate the nail plate at the site of the hematoma with a sharp instrument or the end of a paper clip heated over a fire. This manipulation is painless and instantly relieves tension and, as a result, pain. After evacuation of the hematoma, an aseptic bandage is applied to the finger.
When part or all of the nail plate is torn off without damaging the nail bed, the separated plate is processed and placed in place, secured with a suture. (Fig. 43)

Fig. 43 Refixation of the nail plate
The nail plate is a natural splint for the distal phalanx, a conductor for the growth of new nails and ensures healing of the nail bed with the formation of a smooth surface. If the nail plate is lost, it can be replaced with an artificial nail made from a thin polymer plate, which will provide painless dressings in the future.
Wounds of the nail bed are the most complex injuries, leading in the long term to significant deformation of the nail plate. Such wounds are subject to careful primary surgical treatment with minimal excision of soft tissue, precise comparison of fragments of the nail bed and suture with thin (7\0, 8\0) suture material. The removed nail plate is refixed after treatment. In the postoperative period, immobilization of the phalanx is required for 3-4 weeks to prevent its injury.
Tendon damage.
The choice of tendon reconstruction method is made taking into account the time that has passed since the injury, the prevalence of scar changes along the tendons, and the condition of the skin at the operation site. A tendon suture is indicated when it is possible to connect the damaged tendon end to end and the soft tissue in the area of surgery is in normal condition. There is a primary tendon suture, performed within 10-12 days after the injury in the absence of signs of infection in the wound area and its incised nature, and a delayed suture, which is applied within 12 days to 6 weeks after the injury under less favorable conditions (lacerations and bruises). wounds). In many cases, in a later period, suturing is impossible due to muscle retraction and the occurrence of significant diastasis between the ends of the tendon. All types of tendon sutures can be divided into two main groups - removable and immersed (Fig. 44).

Fig. 44 Types of tendon sutures (a - Bunnell, b - Verdun, c - Cuneo) d - application of an intra-trunk suture, e, f - application of adapting sutures. Stages of suturing in the critical zone.
Removable sutures, proposed in 1944 by Bunnell S., are used to fix the tendon to the bone and in areas where early movements are not so necessary. The suture is removed after the tendon has fused sufficiently firmly with the tissue at the point of fixation. Immersion seams remain in the tissues, bearing a mechanical load. In some cases, additional sutures are used to ensure a more perfect alignment of the ends of the tendons. In old cases, as well as with a primary defect, tendon plasty (tendoplasty) is indicated. The source of tendon autograft is tendons, the removal of which does not cause significant functional and cosmetic disturbances, for example, the tendon of the palmaris longus muscle, the superficial flexor of the fingers, the long extensor of the toes, and the plantaris muscle.
Damage to the finger flexor tendons.
Anatomy.
Flexion of 2-5 fingers is carried out due to two long tendons - superficial, attached to the base of the middle phalanx and deep, attached to the base of the distal phalanx. Flexion of the 1st finger is carried out by the tendon of the long flexor of the 1st finger. The flexor tendons are located in narrow, complex-shaped osteo-fibrous canals that change their shape depending on the position of the finger (Fig. 45)

Fig. 45 Change in the shape of the osteo-fibrous canals of the 2-5 fingers of the hand when they are bent
In places of greatest friction between the palmar wall of the canals and the surface of the tendons, the latter are surrounded by a synovial membrane that forms the sheath. The deep digital flexor tendons are connected through the lumbrical muscles to the extensor tendon apparatus.

Diagnostics.
If the deep digital flexor tendon is damaged and the middle phalanx is fixed, flexion of the nail is impossible; with combined damage to both tendons, flexion of the middle phalanx is also impossible.

Rice. 46 Diagnosis of flexor tendon injuries (1, 3 – deep, 2, 4 – both)
Flexion of the main phalanx is possible due to contraction of the interosseous and lumbrical muscles.
Treatment.
There are five zones of the hand, within which anatomical features influence the technique and results of the primary tendon suture.

Fig.47 Brush zones
In zone 1, only the deep flexor tendon passes through the osteofibrous canal, so its damage is always isolated. The tendon has a small range of motion, the central end is often retained by the mesotenon and can be easily removed without significant expansion of the damaged area. All these factors determine good results from applying a primary tendon suture. The most commonly used transosseous tendon suture is removed. It is possible to use immersed seams.
Throughout zone 2, the tendons of the superficial and deep flexor fingers intersect; the tendons are tightly adjacent to each other and have a large range of motion. The results of tendon suture are often unsatisfactory due to scar adhesions between the sliding surfaces. This zone is called critical or “no man’s land.”
Due to the narrowness of the osteofibrous canals, it is not always possible to suture both tendons; in some cases, it is necessary to excise the superficial flexor tendon of the finger and apply a suture only to the deep flexor tendon. In most cases, this avoids finger contractures and does not significantly affect flexion function.
In zone 3, the flexor tendons of adjacent fingers are separated by neurovascular bundles and lumbrical muscles. Therefore, tendon injuries in this area are often accompanied by damage to these structures. After suture of the tendon, suture of the digital nerves is necessary.
Within zone 4, the flexor tendons are located in the carpal tunnel along with the median nerve, which is located superficially. Tendon injuries in this area are quite rare and are almost always combined with damage to the median nerve. The operation involves dissecting the transverse carpal ligament, suturing the deep digital flexor tendons, and excising the superficial flexor tendons.
Throughout zone 5, the synovial sheaths end, the tendons of adjacent fingers pass close to each other and, when the hand is clenched into a fist, they move together. Therefore, cicatricial fusion of the tendons with each other has virtually no effect on the amount of finger flexion. The results of tendon suture in this area are usually good.
Postoperative management.
The finger is immobilized using a dorsal plaster splint for a period of 3 weeks. From the second week, after the swelling subsides and the pain in the wound decreases, passive flexion of the finger is performed. After removing the plaster splint, active movements begin.
Damage to the extensor tendons of the fingers.
Anatomy.
The formation of the extensor apparatus involves the tendon of the common extensor finger and the tendon of the interosseous and lumbrical muscles, connected by many lateral ligaments, forming a tendon-aponeurotic stretch (Fig. 48, 49)

Fig. 48 Structure of the extensor apparatus of the hand: 1 - Triangular ligament, 2 - attachment point of the extensor tendon, 3 - lateral connection of the collateral ligament, 4 - disc above the middle joint, 5 - spiral fibers, 5 - middle bundle of the long extensor tendon, 7 - lateral bundle of the long extensor tendon, 8 - attachment of the long extensor tendon on the main phalanx, 9 - disc above the main joint, 10 and 12 - long extensor tendon, 11 - lumbrical muscles, 13 - interosseous muscles.
Rice. 49 Extensors of the fingers and hand.
It must be remembered that the index finger and little finger, in addition to the common one, also have an extensor tendon. The middle bundles of the extensor tendon of the fingers are attached to the base of the middle phalanx, extending it, and the lateral bundles are connected to the tendons of the small muscles of the hand, attached to the base of the nail phalanx and perform the function of extending the latter. The extensor aponeurosis at the level of the metacarpophalangeal and proximal interphalangeal joints forms a fibrocartilaginous disc similar to the patella. The function of the small muscles of the hand depends on the stabilization of the main phalanx by the extensor finger. When the main phalanx is bent, they act as flexors, and when extended, together with the extensor fingers, they become extensors of the distal and middle phalanges.
Thus, we can speak of perfect extension-flexion function of the finger only if all anatomical structures are intact. The presence of such a complex interconnection of elements to some extent favors the spontaneous healing of partial damage to the extensor apparatus. In addition, the presence of lateral ligaments of the extensor surface of the finger prevents the tendon from contracting when damaged.
Diagnostics.
The characteristic position that the finger takes depending on the level of damage allows you to quickly make a diagnosis (Fig. 50).

Fig. 50 Diagnosis of damage to the extensor tendons
extensors at the level of the distal phalanx, the finger assumes a flexion position at the distal interphalangeal joint. This deformity is called a “mallet finger.” In most cases of fresh injuries, conservative treatment is effective. To do this, the finger must be fixed in a hyperextended position at the distal interphalangeal joint using a special splint. The amount of hyperextension depends on the patient’s level of joint mobility and should not cause discomfort. The remaining joints of the finger and hand must be left free. The immobilization period is 6-8 weeks. However, the use of splints requires constant monitoring of the position of the finger, the condition of the elements of the splint, as well as the patient’s understanding of the task facing him, therefore, in some cases, transarticular fixation of the nail phalanx with a knitting needle is possible for the same period. Surgical treatment is indicated when the tendon is torn from its attachment site with a significant bone fragment. In this case, a transosseous suture of the extensor tendon is performed with fixation of the bone fragment.
When the extensor tendons are damaged at the level of the middle phalanx, the triangular ligament is simultaneously damaged, and the lateral bundles of the tendon diverge in the palmar direction. Thus, they do not straighten, but bend the middle phalanx. In this case, the head of the main phalanx moves forward through a gap in the extensor apparatus, like a button passing into a loop. The finger assumes a position bent at the proximal interphalangeal joint and hyperextended at the distal interphalangeal joint. This deformation is called a “boutonniere”. With this type of injury, surgical treatment is necessary - suturing the damaged elements, followed by immobilization for 6-8 weeks.
Treatment of injuries at the level of the main phalanx, metacarpophalangeal joints, metacarpus and wrist is only surgical - primary tendon suture followed by immobilization of the hand in the position of extension in the wrist and metacarpophalangeal joints and slight flexion in the interphalangeal joints for a period of 4 weeks with subsequent development of movements.
Damage to the nerves of the hand.
The hand is innervated by three main nerves: the median, ulnar and radial. In most cases, the main sensory nerve of the hand is the median, and the main motor nerve is the ulnar nerve, innervating the muscles of the eminence of the little finger, interosseous, 3 and 4 lumbrical muscles and the adductor pollicis muscle. Of important clinical importance is the motor branch of the median nerve, which arises from its lateral cutaneous branch immediately after exiting the carpal tunnel. This branch innervates the short flexor of the 1st finger, as well as the short abductor and opponor muscles of the Many. the muscles of the hand have double innervation, which preserves to one degree or another the function of these muscles if one of the nerve trunks is damaged. The superficial branch of the radial nerve is the least significant, providing sensation to the dorsum of the hand. If both digital nerves are damaged due to loss of sensitivity, the patient cannot use the fingers and their atrophy occurs.
The diagnosis of nerve damage should be made before surgery, since this is not possible after anesthesia.
Suturing the nerves of the hand requires the use of microsurgical techniques and adequate suture material (6\0-8\0 thread). In case of fresh injuries, soft and bone tissues are first processed, after which the nerve suture is started (Fig. 51)

Fig. 51 Epineural suture of the nerve
The limb is fixed in a position that provides the least tension on the suture line for 3-4 weeks.
Defects of soft tissues of the hand.
Normal hand function is possible only if the skin is intact. Each scar creates an obstacle to its implementation. The skin in the scar area has reduced sensitivity and is easily damaged. Therefore, one of the most important tasks of hand surgery is to prevent scar formation. This is achieved by placing a primary suture on the skin. If, due to a skin defect, it is impossible to apply a primary suture, then plastic replacement is necessary.
In case of superficial defects, the bottom of the wound is represented by well-supplied tissues - subcutaneous fatty tissue, muscle or fascia. In these cases, transplantation of non-vascularized skin grafts gives good results. Depending on the size and location of the defect, split or full-thickness flaps are used. Necessary conditions for successful graft engraftment are: good blood supply to the bottom of the wound, absence of infection and tight contact of the graft with the receiving bed, which is ensured by applying a pressure bandage (Fig. 52)

Fig52 Stages of applying a pressure bandage
The bandage is removed on the 10th day.
Unlike superficial defects, with deep wounds the bottom of the wound is tissue with a relatively low level of blood supply - tendons, bones, joint capsule. For this reason, the use of non-vascularized flaps is ineffective in these cases.
The most common damage is tissue defects of the nail phalanx. There are many methods for covering them with blood-supplied flaps. When detaching the distal half of the nail phalanx, plastic surgery with triangular sliding flaps, which are formed on the palmar or lateral surfaces of the finger, is effective (Fig. 53)

Fig. 53 Plastic surgery with a triangular sliding flap for a skin defect of the nail phalanx

Fig. 54 Plastic surgery using a palmar digital sliding flap
Triangular areas of skin are connected to the finger by a stalk consisting of fatty tissue. If the soft tissue defect is more extensive, then a palmar digital sliding flap is used (Fig. 54)
For defects in the flesh of the nail phalanx, cross flaps from the adjacent longer finger are widely used (Fig. 55), as well as a skin-fat flap of the palmar surface of the hand.
Fig.55 Plastic surgery using a skin-fat flap from the palmar surface of the hand.
The most severe type of hand tissue defect occurs when the skin is removed from the fingers like a glove. In this case, the skeleton and tendon apparatus can be completely preserved. For the damaged finger, a tubular flap on a pedicel is formed (Filatov’s sharp stem); when skeletonizing the entire hand, plastic surgery is performed using skin-fat flaps from the anterior abdominal wall (Fig. 56).

Fig. 56 Plastic surgery of a scalped wound of the middle phalanx using Filatov’s “sharp” stem
Tendon canal stenosis.
The pathogenesis of degenerative-inflammatory diseases of the tendon canals has not been fully studied. Women aged 30-50 years are most often affected. The predisposing factor is static and dynamic overload of the hand.
De Quervain's disease
1 osteofibrous canal and the tendons of the long abductor pollicis muscle and its short extensor muscle passing through it are affected.
The disease is characterized by pain in the area of the styloid process, the presence of a painful lump on it, a positive Finkelstein symptom: acute pain in the area of the styloid process of the radius, occurring when the hand is abducted ulnarly, with 1 finger pre-bent and fixed. (Fig. 57)

Fig. 57 Finkelstein's symptom
X-ray examination makes it possible to exclude other diseases of the wrist joint, as well as to identify local osteoporosis of the apex of the styloid process and hardening of the soft tissues above it.
Treatment.
Conservative therapy involves local administration of steroid drugs and immobilization.
Surgical treatment is aimed at decompressing 1 canal by dissecting its roof.
After anesthesia, a skin incision is made over the painful lump. Just under the skin is the dorsal branch of the radial nerve; it must be carefully retracted to the rear. By making passive movements with the thumb, 1 canal and the site of stenosis are examined. Next, the dorsal ligament and its partial excision are carefully dissected using the probe. After this, the tendons are exposed and inspected, making sure that nothing interferes with their sliding. The operation ends with careful hemostasis and suturing of the wound.
Stenosing ligamentitis of the annular ligaments.
The annular ligaments of the tendon sheaths of the flexor fingers are formed by thickening of the fibrous sheath and are located at the level of the diaphysis of the proximal and middle phalanges, as well as above the metacarpophalangeal joints.
It is still not clear what is primarily affected - the annular ligament or the tendon passing through it. In any case, it is difficult for the tendon to slide through the annular ligament, which leads to “snapping” of the finger.
Diagnosis is not difficult. Patients themselves show a “snapping finger”; a painful lump is palpated at the level of pinching.
Surgical treatment gives a quick and good effect.
The incision is made according to the rules described in the “access to the hand” section. The thickened annular ligament is exposed. The latter is dissected along a grooved probe, and its thickened part is excised. The freedom of tendon gliding is assessed by flexion and extension of the finger. In case of old processes, additional opening of the tendon sheath may be required.
Dupuytren's contracture.
Dupuytren's contracture (disease) develops as a result of cicatricial degeneration of the palmar aponeurosis with the formation of dense subcutaneous cords.
Mostly elderly men (5% of the population) suffer.
Diagnosis usually does not cause difficulties. The disease usually develops over several years. Strands are formed that are painless, dense on palpation and cause limitation of active and passive extension of the fingers. The 4th and 5th fingers are most often affected, and both hands are often affected. (Fig.58)

Fig. 58 Dupuytren's contracture of 4 fingers of the right hand.
Etiology and pathogenesis.
Not exactly known. The main theories are traumatic, hereditary. There is a connection with the proliferation of endothelial cells of the vessels of the palmar aponeurosis and a decrease in oxygen content, which leads to the activation of fibroplastic processes.
Often combined with Ledderhose disease (scarring of the plantar aponeurosis) and fibroplastic induration of the penis (Peyronie's disease).
Anatomy of the palmar aponeurosis.

1. m. palmaris brevis.2. m. palmaris longus.3. volar carpal ligament communis.4. volar carpal ligament proprius.5. Palmar aponeurosis.6. Tendon of palmar aponeurosis.7. Transverse palmar ligament.8. vaginae and ligaments of mm. flexor muscles.9. tendon of m. flexor carpi ulnaris.10.
tendon of m. flexor carpi radialis.
The palmar aponeurosis has the shape of a triangle, the apex of which is directed proximally, and the tendon of the palmaris longus muscle is woven into it. The base of the triangle breaks up into bundles going to each finger, which intersect with the transverse bundles. The palmar aponeurosis is closely connected with the skeleton of the hand and is separated from the skin by a thin layer of subcutaneous fatty tissue.
Classification.
Depending on the severity of clinical manifestations, there are 4 degrees of Dupuytren’s contracture:
1st degree – characterized by the presence of a compaction under the skin that does not limit the extension of the fingers. At this degree, patients usually mistake this lump for “namin” and rarely consult a doctor.
2nd degree. At this degree, finger extension is limited to 30 0
3rd degree. Limitation of extension from 30 0 to 90 0.
4th degree. Extension deficit exceeds 90 0 .
Treatment.
Conservative therapy is ineffective and can be recommended only in the first degree and as a stage of preoperative preparation.
The main method of treating Dupuytren's contracture is surgery.
A large number of operations have been proposed for this disease. The following are of primary importance:
Aponeurectomy– excision of the scarred palmar aponeurosis. It is made from several transverse incisions, which are made according to the rules described in the “incisions on the hand” section. Strands of the altered palmar aponeurosis are isolated and excised subcutaneously. This can damage the common digital nerves, so this step must be performed with extreme care. As the aponeurosis is excised, the finger is gradually removed from the flexion position. The skin is sutured without tension and a pressure bandage is applied to prevent the formation of a hematoma. A few days after the operation, they begin to move the fingers to the extension position using dynamic splints.
The most common injuries to the upper limb are fractures of the radius in the lower third...
The most common injuries to the upper extremity are fractures of the radius in the lower third (radius in a typical location) and fractures in the upper third of the humerus (surgical neck)
rice. 127 Bones of the upper limb ( ossa membri superioris) right; front view.Finger bones (phalanges), ossa digitorum (phalanges) (see Fig. , , , , ), are presented phalanges, phalanges, related in shape to long bones. The first, thumb, finger has two phalanges: proximal, phalanx proximalis, And distal, phalanx distalis. The remaining fingers still have middle phalanx, phalanx media. Each phalanx has a body and two epiphyses - proximal and distal.
Body, corpus, each phalanx is flattened on the anterior (palm) side. The surface of the body of the phalanx is limited on the sides by small scallops. On it is nutrient opening, continuing to distally directed nutrient channel.
The superior, proximal, end of the phalanx, or base, basis phalangis, thickened and has articular surfaces. The proximal phalanges articulate with the bones of the metacarpus, and the middle and distal phalanges are connected to each other.
The lower, distal, end of the 1st and 2nd phalanges has head of the phalanx, caput phalangis.
At the lower end of the distal phalanx, on the back side, there is a slight roughness - tuberosity of the distal phalanx, tuberositas phalangis distalis.
In the area of the metacarpophalangeal joints of the 1st, 2nd and 4th fingers and the interphalangeal joint of the 1st finger on the palmar surface, in the thickness of the muscle tendons, there are sesamoid bones, ossa sesamoidea.
 rice. 151. Bones of the hand, right (x-ray). 1 - radius; 2 - styloid process of the radius; 3 - lunate bone; 4 - scaphoid bone; 5 - trapezium bone; 6 - trapezoid bone; 7-1 metacarpal bone; 8 - sesamoid bone; 9 - proximal phalanx of the thumb; 10 - distal phalanx of the thumb; 11 - II metacarpal bone; 12 - proximal phalanx of the index finger; 13 - base of the middle phalanx of the index finger; 14 - distal phalanx of the index finger; 15 - capitate bone; 16 - hook of the hamate; 17 - hamate bone; 18 - pisiform bone; 19 - triangular bone; 20 - styloid process of the ulna; 21 - head of the ulna.
rice. 151. Bones of the hand, right (x-ray). 1 - radius; 2 - styloid process of the radius; 3 - lunate bone; 4 - scaphoid bone; 5 - trapezium bone; 6 - trapezoid bone; 7-1 metacarpal bone; 8 - sesamoid bone; 9 - proximal phalanx of the thumb; 10 - distal phalanx of the thumb; 11 - II metacarpal bone; 12 - proximal phalanx of the index finger; 13 - base of the middle phalanx of the index finger; 14 - distal phalanx of the index finger; 15 - capitate bone; 16 - hook of the hamate; 17 - hamate bone; 18 - pisiform bone; 19 - triangular bone; 20 - styloid process of the ulna; 21 - head of the ulna. The phalanges of the human fingers have three parts: proximal, main (middle) and terminal (distal). On the distal part of the nail phalanx there is a clearly visible nail tuberosity. All fingers are formed by three phalanges, called the main, middle and nail. The only exception is the thumbs - they consist of two phalanges. The thickest phalanges of the fingers form the thumbs, and the longest ones form the middle fingers.
The phalanges of the fingers belong to the short tubular bones and have the appearance of a small elongated bone, in the shape of a semi-cylinder, with the convex part facing the back of the hand. At the ends of the phalanges there are articular surfaces that take part in the formation of interphalangeal joints. These joints have a block-like shape. They can perform extensions and flexions. The joints are well strengthened by collateral ligaments.
In some chronic diseases of the internal organs, the phalanges of the fingers are modified and take on the appearance of “drumsticks” (spherical thickening of the terminal phalanges), and the nails begin to resemble “watch glasses”. Such modifications are observed in chronic lung diseases, cystic fibrosis, heart defects, infective endocarditis, myeloid leukemia, lymphoma, esophagitis, Crohn's disease, liver cirrhosis, diffuse goiter.
Fractures of the phalanges of the fingers most often occur as a result of a direct blow. A fracture of the nail plate of the phalanges is usually always comminuted.
Clinical picture: the phalanx of the fingers hurts, swells, the function of the injured finger becomes limited. If the fracture is displaced, then the deformation of the phalanx becomes clearly visible. In case of fractures of the phalanges of the fingers without displacement, sprain or displacement is sometimes mistakenly diagnosed. Therefore, if the phalanx of the finger hurts and the victim associates this pain with injury, then an X-ray examination (fluoroscopy or radiography in two projections) is required, which allows making the correct diagnosis.
Treatment of a fracture of the phalanx of the fingers without displacement is conservative. An aluminum splint or plaster cast is applied for three weeks. After this, physiotherapeutic treatment, massage and exercise therapy are prescribed. Full mobility of the damaged finger is usually restored within a month.
In case of a displaced fracture of the phalanges of the fingers, comparison of bone fragments (reposition) is performed under local anesthesia. Then a metal splint or plaster cast is applied for a month.
If the nail phalanx is fractured, it is immobilized with a circular plaster cast or adhesive plaster.
Even the smallest joints in the human body - the interphalangeal joints - can be affected by diseases that impair their mobility and are accompanied by excruciating pain. Such diseases include arthritis (rheumatoid, gout, psoriatic) and deforming osteoarthritis. If these diseases are not treated, then over time they lead to the development of severe deformation of the damaged joints, complete disruption of their motor function and atrophy of the muscles of the fingers and hands. Despite the fact that the clinical picture of these diseases is similar, their treatment is different. Therefore, if the phalanges of your fingers hurt, you should not self-medicate. Only a doctor, after conducting the necessary examination, can make the correct diagnosis and accordingly prescribe the necessary therapy.

The meaning of life is related to the question “What to live for”, and not to the question of how to maintain life. A person's attitude is...

A mushroom is a living organism that forms a separate kingdom of the same name. For a long time they were classified as part of the plant kingdom. But in...

For lovers of “quiet” hunting, mushroom season begins in early summer and lasts until late autumn. And rarely do they...
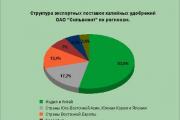
Aleshnikova, V.I. Use of professional consultants. - M.: Infra-M, 1999. - 240 p. 2. Beich, E....

Orange juice. The symbolic meaning of orange juice in dream books is pleasure and temptation. Quite often we...

We most often overcome all kinds of difficulties encountered along the path of life. Of course, for this we make...

This year your patron Neptune will be in your constellation and this is a good sign, because you will...

1993 who? 1993 is the year of which animal? — According to the Chinese horoscope, 1873, 1933, 1993 belonged to the years of the Black...

Wave-particle duality of light means that light simultaneously has the properties of continuous...

The role of biology is enormous in our world. Although it is not one of the priority subjects, most schoolchildren and...

Amines are organic derivatives of ammonia containing an NH 2 amino group and an organic radical. In general...

How to answer questions in Part BThe second part of the social studies work consists of 7 tasks with a short answer....

Form TORG-15 is drawn up in the case when during transportation, movement between and within the warehouse, when...

Nutritionists say that for good health and a slim figure, you must include snacks in your...

A mushroom is a living organism that forms a separate kingdom of the same name. For a long time they were classified as a kingdom...

For lovers of “quiet” hunting, mushroom season begins in early summer and lasts until late autumn. And rarely do they...