Dream interpretation of a dead man being alive
Dream interpretation is an ancient art that allows you to at least assess the psychological status of a person, because...
Postpartum parametritis is a purulent-infiltrative lesion of the pelvic tissue. As a complication of the postpartum period, parametritis is currently quite rare. The pelvic tissue becomes infected through the lymphogenous route, and the inflammatory process spreads along the veins and lymphatic vessels.
The microflora with parametritis, as with other forms of postpartum infection, is mixed. The predominant pathogens are E.coli, Klebsiella, Proteus. Non-spore-forming anaerobes, streptococci and staphylococci, are often isolated.
Predisposing factors for the development of parametritis most often are:
There are three main stages in the development and progression of parametritis:
The disease usually begins on the 7-10th day after birth. Accompanied by chills with an increase in body temperature to 38-39 0 C. The patient complains of constant pain in the lower abdomen, in the left or right iliac region, radiating to the sacrum and lumbar region. When an abscess threatens to break through into the bladder, pain during urination and pyuria are observed, and into the rectum - tenesmus and diarrhea.
A feature of the clinical picture of upper lateral parametritis is the possibility of the appearance of thromboembolic symptoms associated with periphlebitis of the external iliac vein and its thrombosis.
IN diagnostics of this disease, you should first of all pay attention to the clinical picture and complaints of the patient.
Bimanual examination reveals infiltration and sharp pain on palpation of the affected parametrium; the lateral vault of the vagina is sharply shortened; the cervix is located asymmetrically relative to the midline and is displaced in the direction opposite to the affected parametrium; displacement of the pelvic organs is difficult; the uterus is not palpable separately; a conglomerate of formations is determined (uterus, appendages and adjacent organs).
It is mandatory to conduct a rectovaginal examination, which evaluates the prolapse of the infiltrate or abscess towards the rectum, as well as the condition of the mucous membrane above the infiltrate (mobile, limited mobility, immobile).
The complex of diagnostic measures necessarily includes a clinical blood test, a biochemical blood test, a coagulogram, a general urine test, and a bacteriological examination.
Ultrasound becomes important in the diagnosis of postpartum parametritis. On an echogram, inflammatory infiltrates are determined in the form of echo-positive formations of irregular shape without clear contours and capsule. Infiltrates are characterized by reduced echogenicity in relation to surrounding tissues and, when suppurating, contain cystic formations in their structure with a clear capsule and thick heterogeneous content. Among other instrumental diagnostic methods, it is advisable to use CT and echography of the kidneys.
Complex treatment postpartum parametritis is generally similar to the treatment of postpartum endomyometritis and includes: antibacterial therapy, antifungal antibiotics, infusion therapy, desensitizing therapy, immunocorrective therapy, improvement of microcirculation, correction of vaginal microbiocenosis.
If an abscess forms in the parametrium, then surgical treatment with opening and drainage of the abscess through vaginal access is necessary.
Is something bothering you? Do you want to know more detailed information about Postpartum parametritis, its causes, symptoms, methods of treatment and prevention, the course of the disease and diet after it? Or do you need an inspection? You can make an appointment with a doctor– clinic Eurolab always at your service! The best doctors will examine you, study external signs and help you identify the disease by symptoms, advise you and provide the necessary assistance and make a diagnosis. you also can call a doctor at home. Clinic Eurolab open for you around the clock.
How to contact the clinic:
Phone number of our clinic in Kyiv: (+38 044) 206-20-00 (multi-channel). The clinic secretary will select a convenient day and time for you to visit the doctor. Our coordinates and directions are indicated. Look in more detail about all the clinic’s services on it.
(+38 044) 206-20-00
If you have previously performed any research, Be sure to take their results to a doctor for consultation. If the studies have not been performed, we will do everything necessary in our clinic or with our colleagues in other clinics.
You? It is necessary to take a very careful approach to your overall health. People don't pay enough attention symptoms of diseases and do not realize that these diseases can be life-threatening. There are many diseases that at first do not manifest themselves in our body, but in the end it turns out that, unfortunately, it is too late to treat them. Each disease has its own specific signs, characteristic external manifestations - the so-called symptoms of the disease. Identifying symptoms is the first step in diagnosing diseases in general. To do this, you just need to do it several times a year. be examined by a doctor, in order not only to prevent a terrible disease, but also to maintain a healthy spirit in the body and the organism as a whole.
If you want to ask a doctor a question, use the online consultation section, perhaps you will find answers to your questions there and read self care tips. If you are interested in reviews about clinics and doctors, try to find the information you need in the section. Also register on the medical portal Eurolab to keep abreast of the latest news and information updates on the site, which will be automatically sent to you by email.
| Obstetric peritonitis in the postpartum period |
| Anemia in pregnancy |
| Autoimmune thyroiditis during pregnancy |
| Fast and rapid birth |
| Management of pregnancy and childbirth in the presence of a scar on the uterus |
| Chickenpox and herpes zoster in pregnant women |
| HIV infection in pregnant women |
| Ectopic pregnancy |
| Secondary weakness of labor |
| Secondary hypercortisolism (Itsenko-Cushing's disease) in pregnant women |
| Genital herpes in pregnant women |
| Hepatitis D in pregnant women |
| Hepatitis G in pregnant women |
| Hepatitis A in pregnant women |
| Hepatitis B in pregnant women |
| Hepatitis E in pregnant women |
| Hepatitis C in pregnant women |
| Hypocorticism in pregnant women |
| Hypothyroidism during pregnancy |
| Deep phlebothrombosis during pregnancy |
| Discoordination of labor (hypertensive dysfunction, uncoordinated contractions) |
| Adrenal cortex dysfunction (adrenogenital syndrome) and pregnancy |
| Malignant breast tumors during pregnancy |
| Infections caused by group A streptococci in pregnant women |
| Infections caused by group B streptococci in pregnant women |
| Iodine deficiency diseases during pregnancy |
| Candidiasis in pregnant women |
| C-section |
| Cephalohematoma due to birth trauma |
| Rubella in pregnant women |
| Criminal abortion |
| Cerebral hemorrhage due to birth trauma |
| Bleeding in the afterbirth and early postpartum periods |
| Lactation mastitis in the postpartum period |
| Leukemia during pregnancy |
| Lymphogranulomatosis during pregnancy |
| Skin melanoma during pregnancy |
| Mycoplasma infection in pregnant women |
| Uterine fibroids during pregnancy |
| Miscarriage |
| Non-developing pregnancy |
| Failed miscarriage |
| Quincke's edema (fcedema Quincke) |
| Parvovirus infection in pregnant women |
| Paresis of the diaphragm (Cofferat syndrome) |
| Facial nerve paresis during childbirth |
| Pathological preliminary period |
| Primary weakness of labor |
| Primary aldosteronism during pregnancy |
| Primary hypercortisolism in pregnant women |
| Bone fracture due to birth trauma |
| Post-term pregnancy. Delayed birth |
| Damage to the sternocleidomastoid muscle due to birth trauma |
| Postpartum adnexitis |
| Postpartum thyroiditis |
| Postpartum endometritis |
| Placenta previa |
| Placenta previa |
Postpartum parametritis- this is a purulent-infiltrative lesion of the pelvic tissue. As a complication of the postpartum period, parametritis is currently quite rare. The pelvic tissue becomes infected through the lymphogenous route, and the inflammatory process spreads along the veins and lymphatic vessels.
The microflora with parametritis, as with other forms of postpartum infection, is mixed. Among the pathogens, E. coli, Klebsiella, and Proteus predominate. Non-spore-forming anaerobes, streptococci and staphylococci, are often isolated.
Depending on the topography of the pelvic tissue, anterior, lateral and posterior parametritis are distinguished.
The disease usually begins 7-10 days after birth.
If an abscess forms during parametrium, surgical treatment with opening and drainage of the abscess through vaginal access is necessary.
Parametritis - inflammation of the periuterine tissue - usually occurs with lymphogenous spread of infection. The infection penetrates the periuterine tissue either through the intact wall of the uterus, or through ruptures in the vagina, cervix or uterine body, which allow microbes access to the tissue.
A feature of inflammation of fiber is the poor ability of this tissue to delimit the inflammatory process.
Therefore, anatomical conditions (direction of lymphatic and blood vessels, the presence of fibrous formations delimiting the tissue into sections) are of significant importance in the spread and localization of the inflammatory process in the tissue.
Anatomically, the pelvic tissue is divided into four large sections: the anterior - peri-vesical, posterior - pararectal and two lateral - peri-uterine (parametric). Inflammation of the tissue in the anterior section is called paravesicitis.
Paravesicitis can occur during the transition of inflammation from the lateral sections of the tissue, as well as initially. In the latter case, the entry point for infection is the anterior part of the cervix or the mucous membrane of the bladder.
The posterior section of the fiber is located in the rectum area. The uterosacral ligaments divide it into two parts - the upper and lower sections.
In the upper section, fiber is located between the rectum and the sacrum; in the lower section, it surrounds the rectum on all sides, forming a partition in front between the vagina and the intestine.
Inflammation of the fiber of the lower section is caused by the spread of infection from the vagina or rectum and is called paracolpitis or paraproctitis.
Each of the lateral sections of the fiber is divided into two more sections - the upper, enclosed between the closely adjacent peritoneal layers of the broad uterine ligaments and containing a small amount of loose fiber, and the lower, containing a powerful accumulation of connective tissue bundles with an admixture of muscle elements (lig. cardinale uteri) . The infection usually penetrates into the upper section from the body of the uterus, from the placental area, into the lower section - most often from the cervix when it is ruptured on the sides. Depending on the damage to the upper or lower part of the periuterine tissue, upper or lower parametritis is distinguished.
In addition to the four large sections of fiber, there are two more small sections in the pelvis - precervical and retrocervical. They are like a connecting link between large departments. Inflammation of the fiber of these sections is called anterior and posterior parametritis.
Only at the beginning of the disease or with a relatively mild form of infection is the inflammatory process localized within one of the sections of the pelvic tissue. During a severe inflammatory process, the plates of compacted fiber separating one section from another are destroyed and the process affects neighboring sections.
The pathological picture of parametritis does not differ significantly from ordinary inflammation of the tissue. The inflammatory effusion is initially serous in nature, but soon becomes serous-fibrinous. The amount of fibrin in it increases, fibrin loss occurs, and the inflammatory effusion thickens. A small cell infiltrate forms around the inflammatory focus.
Thrombosis develops in dilated lymphatic vessels. All this to a certain extent contributes to the localization of the process. Subsequently, a dense connective tissue (granulation) membrane is formed on the periphery of the affected area, delimiting the inflammatory focus.
The inflammatory infiltrate formed during parametritis gradually resolves or undergoes suppuration.
Parametritis usually begins on the 10-12th day after birth with chills and a rise in temperature to 39-40°. Parametritis is usually preceded by endomyometritis. Often, before the temperature rises, there is a decrease in temperature due to the course of endomyometritis.
The temperature curve for parametritis is relatively constant with remissions of 0.5-1°C. The patient's general condition suffers relatively little; complaints are usually limited to mild nagging pain in the lower abdomen.
Severe pain is observed either at the very beginning of the disease - with irritation of the peritoneum covering the affected part of the pelvic tissue, or when the pathological process transitions to suppuration. Disturbances in the function of adjacent organs occur with appropriate localization of the infiltrate.
When it is located in the anterior section of the pelvic tissue, around the bladder, painful, frequent urination or retention is observed; when localized in the posterior section, around the rectum, there is difficulty defecating.
At the very beginning of the disease, local symptoms are mild. An internal examination reveals swelling and pastiness in the area of the tissue affected by inflammation.
After 2-3 days, the infiltrate begins to clearly contour, which initially has a doughy and then dense consistency. Depending on the location of the infiltrate, its shape and location vary. The most common type of parametritis is lateral parametritis.
In this disease, the infiltrate is located between the lateral surface of the uterus and the pelvic wall, displaces the uterus to the opposite side, reaches the lateral wall of the pelvis, passing onto it with a wide wing.
The lateral fornix becomes flattened, its mucous membrane loses mobility due to infiltration of the vaginal wall. With bilateral lateral parametritis, the uterus appears to be walled up in the infiltrate.
Sometimes with lateral parametritis, only the upper or only the lower part of the parametrium is affected. With upper lateral parametritis, the infiltrate, located in the upper part of the broad ligament, tilts the uterus in the opposite direction and “dresses the uterus as if with a hood” (V. Ya. Ilkevich). With isolated inflammation of the lower section, the uterus tilts towards the side affected by the inflammation.
The infiltrate can spread in different directions. Most often, it spreads anteriorly and, having emerged from the pelvic cavity, is palpated from the outside in the form of a dense formation located above the Pupart ligament, often above the superior anterior iliac spines.
Due to the extraperitoneal location of the infiltrate, the upper palpation (i.e.
determined by palpation) and upper percussion (determined by percussion) boundaries coincide; with percussion of the superior anterior iliac spines on the affected side, dullness of tone is obtained (Genter's symptom).
When inflammation passes to the peri-vesical tissue, the infiltrate, spreading along the posterior surface of the anterior abdominal wall, takes on a triangular shape (a triangle with the apex facing the navel); the abdominal wall gives the impression of a starched shirtfront (plastron abdominal).
With inflammation of the posterior part of the periuterine tissue above the posterior vaginal fornix, a dense flat infiltrate is determined, which spreads posteriorly and covers the rectum, often narrowing its lumen.
When the infiltrate is localized on the surface of the lumbar muscle (parapsoitis), the patient takes a forced position on her back with her leg abducted and bent at an angle.
The course of parametritis varies. Sometimes the febrile period lasts 1-2 weeks and the temperature drops critically or lytically, sometimes the febrile period drags on to 4-5 weeks. In some cases, the temperature is low-grade and the parametritis is sluggish. Resorption of the infiltrate also does not occur with the same speed.
Relatively rarely, with parametritis, suppuration is observed (at the 3-5th week of the disease).
An abscess of periuterine tissue most often forms in the lateral parametrium or in the tissue behind the uterus. Relatively rarely, an abscess occurs in the retrocervical or prevesical tissue.
With suppuration, the temperature becomes remitting. The infiltrate softens and fluctuation appears.
If the abscess is not opened in time, the pus will come out along the paths that connect the pelvic tissue with the outer tissue of the body, or will break into adjacent hollow organs.
Suppuration of the periuterine tissue can spread: 1) over the Pupart's ligament; 2) through the sciatic foramen along the course of a. glutea or a. ischiadic" etc.
ischiadicus under the gluteal muscles; 3) under the Poupart ligament through the lacuna vasorum to the thigh; 4) in the perinephric region; 5) through the obturator foramen (rarely); 6) through the lesser sciatic foramen into the sciatic rectal space (rarely). The most dangerous is the spread of suppuration to the perinephric area.
At the site of a threatening breakthrough of the abscess, a protrusion is usually first observed, then redness of the skin and fluctuation. The resulting abscess can open into the bladder, rectum, or less often into the vagina. With a threatening breakthrough of the abscess into the bladder, severe tenesmus occurs, with a breakthrough into the rectum - tenesmus and diarrhea.
In some cases of the disease, multiple finely cellular purulent foci are formed. A long-term suppurative process develops, which leads to exhaustion of the patient (wound exhaustion). Patients usually die from dystrophy, especially in connection with associated bronchopneumonia; Amyloid degeneration of parenchymal organs (kidneys, liver, spleen) is relatively rare.
Parametritis should be distinguished: 1) as an independent form of the disease (primary parametritis); 2) as a reactive inflammation of fiber during inflammation of the uterine appendages, with thrombophlebitis (secondary parametritis); 3) as a partial manifestation of septic infection.
The use of antibiotics has led to the fact that parametritis as an independent form of the disease is now rare, while mild abortive forms of the disease are usually observed, occurring with low-grade fever and the formation of relatively small infiltrates, which are subsequently reabsorbed.
However, with late prescription of antibiotics, the possibility of transition of the infiltrative process into suppuration, which can clinically occur atypically, cannot be excluded. The main sign of this complication is the appearance of more or less distinct softening in certain areas of the infiltrate.
At the same time, there is a deterioration in the patient’s general condition, an increase in temperature, an increase in leukocytosis, a shift in the leukocyte formula to the left, and an acceleration of ROE.
Treatment of parametritis is mainly carried out according to the provisions set out in the chapter “General principles of treatment of postpartum diseases”.
A parametric abscess must be opened in a timely manner. However, recognizing an abscess is not always easy, especially if there are small purulent foci. In doubtful cases, a test puncture is used to clarify the diagnosis.
Surgical treatment of purulent parametritis consists of extraperitoneal opening of the abscess. The success of treatment largely depends on timely surgical intervention.
You should operate at the first signs of softening of the infiltrate - provided that the abscess is accessible for opening without much risk. Sometimes it is advisable to wait until the abscess becomes more accessible. Often, a puncture is used to clarify the location of the abscess.
With purulent lateral parametritis, the abscess most often extends above the Pupart ligament. In some cases, usually when surgery is overdue, it is enough to cut the skin to open the abscess.
For an operation performed in a timely manner, a layer-by-layer incision (5-6 cm long) is used.
After dissection of the aponeurosis, the abscess is most often approached in a blunt manner, and a puncture of the purulent focus is often performed and a needle is used to penetrate it.
During the operation, it is necessary to take into account the topography of the blood vessels of the lower anterior abdominal wall. Approximately on a line running from the middle of the Poupart ligament upward, between the subcutaneous tissue and the aponeurosis, the superficial epigastric artery will be found during the incision, and on a line passing 2 cm inward from the first, between the transverse fascia and the peritoneum, the inferior epigastric artery.
For a highly and laterally located abscess, the incision is made parallel to the Pupart ligament (2 cm above it), the incision begins outward from the line running from the middle of the Pupart ligament, and leads towards the anterior superior iliac spine. There are no epigastric vessels in this area.
For an abscess, the upper border of which is determined above the medial half of the Pupart ligament, an incision is made in this place - it is made parallel to the ligament (2 cm above it), in the direction from its middle to the pubic tubercle. The vessels in this area must be carefully ligated. If it is impossible to bandage them in isolation, then piercing sutures are used.
If, with lateral parametritis, the abscess is located low and adjacent to the vagina, first make a transverse incision in the area of the posterior vaginal fornix close to the posterior surface of the cervix and then make a path to the abscess using a blunt method.
With anterior parametritis, the infiltrate is located directly behind the anterior abdominal wall.
A puncture is made along the midline in the place of greatest dullness of percussion sound and then, without removing the needle, a longitudinal incision is made, extending it, if necessary, towards the pubis.
The puncture puncture and incision should not be too deep due to the risk of penetration into the abdominal cavity and injury to the intestines and a distended bladder immured in the infiltrate.
In case of purulent posterior parametritis, stepping back slightly from the posterior lip of the cervix, a transverse or semilunar incision is made in the vaginal wall in the area of the posterior vaginal fornix, bluntly moving towards the abscess, puncturing it and opening it with a needle, also bluntly. The abscess located between the bladder and the anterior surface of the uterus is opened through a transverse incision in the area of the anterior vaginal fornix. This operation should only be performed by an experienced obstetrician-gynecologist.
Operations for purulent parametritis, depending on their characteristics, are performed either under general anesthesia using a mixture of ether with oxygen or nitrous oxide, or under local anesthesia.
The surgical incision must be large enough to ensure good drainage of pus from the abscess cavity.
After emptying the abscess, its cavity is washed with hydrogen peroxide and a solution of furatsilin (1:5000) or a solution of monomycin (250,000-500,000 units per 1 liter of 0.25% novocaine solution).
After washing the purulent cavity with a solution of monomycin, this drug is injected into the cavity itself (250,000-500,000 units in 20 ml of 0.5% novocaine solution). The abscess cavity is usually drained using gauze swabs or drainage tubes.
Source: http://www.medical-enc.ru/poslerodov/parametrit.shtml

Postpartum (puerperal) infections are purulent-inflammatory diseases pathogenetically caused by pregnancy and childbirth.
They include wound infections (postpartum ulcers, endometritis), infections limited to the pelvic cavity (metritis, parametritis, salpingoophoritis, pelvioperitonitis, metrothrombophlebitis, etc.
), diffuse infections (peritonitis, progressive thrombophlebitis) and generalized infections (septic shock, sepsis). The time frame during which these complications can develop is from the moment of discharge of the placenta to the end of the sixth week of the postpartum period.
Puerperal diseases of infectious etiology occur in 2-10% of postpartum women. Septic complications play a leading role in the structure of maternal mortality, which puts them among the priority problems of obstetrics and gynecology.
The occurrence of postpartum infections is caused by the penetration of microbial agents through wound surfaces formed as a result of childbirth.
The entrance gates can be ruptures of the perineum, vagina and cervix; the inner surface of the uterus (placental site), postoperative scar during cesarean section.
In this case, pathogens can enter the wound surface both from the outside (from instruments, hands and clothing of personnel, surgical linen, care items, etc.) and from endogenous foci as a result of activation of their own opportunistic flora.
The etiological structure of postpartum infections is very dynamic and variable.
Of the opportunistic microorganisms, aerobic bacteria predominate (enterococci, Escherichia coli, staphylococci, group B streptococci, Klebsiella, Proteus), but anaerobes (fusobacteria, bacteroides, peptostreptococci, peptococci) are also quite common.
The importance of specific pathogens is great - chlamydia, mycoplasmas, fungi, gonococci, trichomonas. A feature of postpartum infections is their polyetiology: in more than 80% of observations, microbial associations are sown, which are more pathogenic and resistant to antibiotic therapy.
The risk of developing postpartum infections is significantly increased in women with pathologies of pregnancy (anemia, toxicosis) and childbirth (early release of water, weak labor, prolonged labor, bleeding, retention of parts of the placenta, lochiometer, etc.), extragenital pathology (tuberculosis, obesity, diabetes diabetes).
Endogenous factors predisposing to microbial contamination of the birth canal can be vulvovaginitis, colpitis, cervicitis, pyelonephritis, tonsillitis, and sinusitis in a postpartum woman.
When infected with highly virulent flora or a significant decrease in the immune mechanisms of a postpartum woman, the infection can spread beyond the primary focus by hematogenous, lymphogenous, intracanalicular, and perineural routes.
Based on the anatomical, topographical and clinical approach, 4 stages of progression of postpartum infection are distinguished (authors: S. V. Sazonova, A. V. Bartels).
1st stage– local infection that does not spread beyond the area of the wound surface (postpartum ulcer of the perineum, vagina and uterine wall, suppuration of sutures, suppuration of hematomas, postpartum endometritis)
2nd stage– postpartum infection that extends beyond the boundaries of the wound surface, but is limited to the pelvic cavity (metroendometritis, adnexitis, parametritis, metrothrombophlebitis, limited pelvic thrombophlebitis, pelvioperitonitis)
3rd stage– diffuse postpartum infection (peritonitis, progressive thrombophlebitis)
4th stage– generalized septic infection (sepsis, infectious-toxic shock).
Lactation mastitis is isolated as a separate form of postpartum infection. The severity of infectious complications after childbirth depends on the virulence of the microflora and the reactivity of the macroorganism, therefore the course of the disease varies from mild and erased forms to severe and fatal cases.
Postpartum ulcer is formed as a result of infection of abrasions, cracks and tears in the skin of the perineum, vaginal mucosa and cervix. The clinical picture of this postpartum complication is dominated by local symptoms, the general condition is usually not disturbed, and the temperature does not exceed low-grade levels.
The postpartum woman complains of pain in the suture area, sometimes itching and dysuria. When examining the birth canal, an ulcer with clear boundaries, local swelling and inflammatory hyperemia is detected. At the bottom of the ulcer, a grayish-yellow coating, areas of necrosis, and mucopurulent discharge are detected.
The ulcer bleeds easily on contact.
Postpartum endometritis(metroendometritis) among other postpartum infections occurs most often - in 36-59% of cases. There are classic, erased, abortive forms and metroendometritis after cesarean section.
In the typical (classical) version, postpartum endometritis manifests itself 3-5 days after birth with an increase in temperature to 38-39 ° C and chills. Locally, subinvolution of the uterus, its pain on palpation, and cloudy, purulent discharge from the cervical canal with a foul odor are noted.
The abortive form of postpartum infection develops on days 2-4, but undergoes rapid reversal due to the start of therapy. For the erased course of postpartum endometritis, a late onset (5-8 days), a protracted or wave-like course, and less pronounced symptoms are typical.
Clinical manifestation of endometritis after delivery by cesarean section occurs on days 1-5; the pathology occurs with general and local manifestations.
It develops on days 10–12 when the infection passes to the parametrium - peri-uterine tissue. A typical clinical presentation includes chills, febrile fever that lasts 7-10 days, and intoxication. The postpartum woman is bothered by pain in the iliac region on the side of inflammation, which gradually increases and radiates to the lower back and sacrum.
A few days after the onset of postpartum infection, a painful infiltrate of first soft and then dense consistency, adherent to the uterus, is palpated in the area of the lateral surface of the uterus. The outcome of postpartum parametritis can be resorption of the infiltrate or its suppuration with the formation of an abscess.
Spontaneous opening of an abscess can occur in the vagina, bladder, uterus, rectum, and abdominal cavity.
Postpartum thrombophlebitis may affect superficial and deep veins. In the latter case, the development of metrothrombophlebitis, thrombophlebitis of the veins of the lower extremities and pelvic veins is possible. Usually appear within 2-3 weeks after birth.
Clinical harbingers of postpartum complications of this type are prolonged fever; persistent step-like increase in heart rate; pain in the legs when moving and pressing on soft tissues; swelling in the ankles, legs or thighs; cyanosis of the lower extremities. The development of metrothrombophlebitis is indicated by tachycardia up to 100 beats/min.
Subinvolution of the uterus, prolonged bleeding, palpation of painful cords along the lateral surfaces of the uterus. Thrombophlebitis of the pelvic veins is dangerous due to the development of ileofemoral venous thrombosis and pulmonary embolism.
Postpartum pelvioperitonitis, or inflammation of the pelvic peritoneum, develops 3-4 days after birth. The manifestation is acute: body temperature quickly increases to 39-40°C, sharp pain appears in the lower abdomen.
Vomiting, flatulence, and painful bowel movements may occur. The anterior abdominal wall is tense, the uterus is enlarged.
Postpartum infection is resolved by resorption of the infiltrate in the pelvis or the formation of an abscess in the pouch of Douglas.
The clinical picture of diffuse and generalized postpartum infection (peritonitis, sepsis) does not differ from that of infectious diseases of other etiologies. Lactation mastitis is discussed in detail in the section “Diseases of the mammary glands”.
Factors indicating the development of postpartum infections are signs of infectious-purulent inflammation in the area of the birth wound or pelvic organs, as well as general septic reactions that occurred in the early period after childbirth (up to 6-8 weeks).
Complications such as postpartum ulcers, suppuration of sutures or hematomas are diagnosed based on a visual examination of the birth canal. A vaginal examination allows a gynecologist to suspect postpartum pelvic infections.
In these cases, slow contraction of the uterus, its soreness, pastiness of the periuterine space, infiltrates in the pelvis, and cloudy, foul-smelling discharge from the genital tract are usually detected.
Additional data is obtained during gynecological ultrasound. In case of suspected thrombophlebitis, Dopplerography of the pelvic organs and Doppler ultrasound of the veins of the lower extremities are indicated.
For postpartum endometritis, hysteroscopy is informative; for purulent parametritis - puncture of the posterior vaginal vault.
According to indications, radiation diagnostic methods are used: phlebography, hysterography, radioisotope study.
All clinical forms of postpartum infection are characterized by a change in the peripheral blood picture: significant leukocytosis with a neutrophilic shift to the left, a sharp increase in ESR. In order to identify infectious agents, bacterial culture of the genital tract and uterine contents is performed.
Histological examination of the placenta may indicate signs of inflammation and, therefore, a high likelihood of developing postpartum infections. An important role in planning therapy and assessing the severity of complications is the study of blood biochemistry, acid-base balance, blood electrolytes, and coagulogram.
The entire range of therapeutic measures for postpartum infections is divided into local and general. Bed rest and applying ice to the abdomen helps stop the infection from spreading further from the pelvic cavity.
Local procedures include treating wounds with antiseptics, dressings, ointment applications, removing sutures and opening the wound when it suppurates, removing necrotic tissue, and local application of proteolytic enzymes.
In case of postpartum endometritis, curettage or vacuum aspiration of the uterine cavity may be required (if placental tissue and other pathological inclusions are retained in it), dilation of the cervical canal, and aspiration and lavage drainage.
When a parametrium abscess forms, it is opened through the vagina or by laparotomy and the periuterine tissue is drained.
Local measures for postpartum infections are carried out against the background of intensive general therapy.
First of all, antibacterial agents are selected that are active against all isolated pathogens (broad-spectrum penicillins, cephalosporins, aminoglycosides and others), which are administered intramuscularly or intravenously in combination with metronidazole.
It is advisable to interrupt breastfeeding during treatment. In order to detoxify and eliminate water-salt imbalance, infusions of colloidal, protein, and saline solutions are used. It is possible to carry out extracorporeal detoxification: hemosorption, lymphosorption, plasmapheresis.
For postpartum infections of staphylococcal etiology, antistaphylococcal gamma globulin, staphylococcal toxoid, and antistaphylococcal plasma are used to increase specific immunological reactivity.
To prevent thrombosis, anticoagulants, thrombolytics, and antiplatelet agents are prescribed under the control of a coagulogram. Antihistamines, vitamins, and glucocorticoids are widely used in the complex of drug therapy.
At the rehabilitation stage, laser therapy, local ultraviolet radiation, UHF therapy, ultrasound, electrical stimulation of the uterus, balneotherapy and other methods of physiotherapy are prescribed.
In some cases, surgical assistance may be required - removal of the uterus (hysterectomy) when it purulently melts; thrombectomy, embolectomy or phlebectomy – for thrombophlebitis.
For wound infections and infections limited to the pelvic area, the prognosis is satisfactory. Timely and adequate therapy can stop further progression of postpartum infections.
However, in the long term, the prognosis for reproductive function can be variable.
The most severe consequences for the health and life of the postpartum mother entail diffuse peritonitis, sepsis and septic shock.
Prevention of postpartum infections is ensured by strict and strict adherence to the sanitary and hygienic regime in maternity institutions, the rules of asepsis and antisepsis, and personal hygiene of personnel. Sanitation of endogenous infection at the stage of pregnancy planning is important.
Source: http://www.krasotaimedicina.ru/diseases/zabolevanija_gynaecology/postpartum-infections
It is a purulent-infiltrative lesion of the pelvic tissue. As a complication of the postpartum period, parametritis is currently quite rare. The pelvic tissue becomes infected through the lymphogenous route, and the inflammatory process spreads along the veins and lymphatic vessels.
The microflora with parametritis, as with other forms of postpartum infection, is mixed. Among the pathogens, E. coli, Klebsiella, and Proteus predominate. Non-spore-forming anaerobes, streptococci and staphylococci, are often isolated.
Predisposing factors for the development of parametritis most often are:
There are three main stages in the development and progression of parametritis:
The disease usually begins on the 7-10th day after birth. Accompanied by chills with an increase in body temperature to 38-390C.
The patient complains of constant pain in the lower abdomen, in the left or right iliac region, radiating to the sacrum and lumbar region.
With a threatening breakthrough of an abscess into the bladder, pain during urination and pyuria are observed, and in the rectum - tenesmus and diarrhea.
A feature of the clinical picture of upper lateral parametritis is the possibility of the appearance of thromboembolic symptoms associated with periphlebitis of the external iliac vein and its thrombosis.
IN diagnostics of this disease, you should first of all pay attention to the clinical picture and complaints of the patient.
Bimanual examination reveals infiltration and sharp pain on palpation of the affected parametrium; the lateral vault of the vagina is sharply shortened; the cervix is located asymmetrically relative to the midline and is displaced in the direction opposite to the affected parametrium; displacement of the pelvic organs is difficult; the uterus is not palpable separately; a conglomerate of formations is determined (uterus, appendages and adjacent organs).
It is mandatory to conduct a rectovaginal examination, which evaluates the prolapse of the infiltrate or abscess towards the rectum, as well as the condition of the mucous membrane above the infiltrate (mobile, limited mobility, immobile).
The complex of diagnostic measures necessarily includes a clinical blood test, a biochemical blood test, a coagulogram, a general urine test, and a bacteriological examination.
Ultrasound becomes important in the diagnosis of postpartum parametritis. On an echogram, inflammatory infiltrates are determined in the form of echo-positive formations of irregular shape without clear contours and capsule.
Infiltrates are characterized by reduced echogenicity in relation to surrounding tissues and, when suppurating, contain cystic formations in their structure with a clear capsule and thick heterogeneous content.
Among other instrumental diagnostic methods, it is advisable to use CT and echography of the kidneys.
Complex treatment postpartum parametritis is generally similar to the treatment of postpartum endomyometritis and includes: antibacterial therapy, antifungal antibiotics, infusion therapy, desensitizing therapy, immunocorrective therapy, improvement of microcirculation, correction of vaginal microbiocenosis.
If an abscess forms in the parametrium, then surgical treatment with opening and drainage of the abscess through vaginal access is necessary.
Mental and behavioral disorders associated with the postpartum period, Disorder of adaptive reactions, Bleeding in the placenta and early postpartum periods, Postinjection lipodystrophy, Dysfunction of the sphincter of Oddi (postcholecystectomy syndrome), Obstetric peritonitis in the postpartum period, Postcommotion syndrome, Syndrome after total oophorectomy, Postgastroresection disorders, Lactation mastitis in the postpartum period
Postpartum parametritis is a purulent lesion of the parametric tissue of the pelvis. It occurs as a complication of the birth process as a result of infection of the tissue in a lymphogenous manner, through the veins and lymphatic vessels. The causes of the development of the disease are birth injuries of the uterus I-III degrees, incorrect treatment of postpartum ulcers or endometritis, postpartum thrombophlebitis of the parametrium.
The disease develops 8-10 days after delivery. It is characterized by chills, temperature up to 39C, pain in the abdomen, in the right or left iliac region, radiating to the lumbar region and sacrum. In case of a threatening breakthrough of an abscess into the rectum, tenesmus and diarrhea are observed, in the bladder - painful urination, pyuria. With upper lateral parametritis, thromboembolic symptoms occur due to thrombosis of the external iliac vein.
The development of postpartum parametritis is divided into three stages: exudation (hyperemia, serous impregnation of tissues), infiltration (formation of infiltrate), suppuration (formation of microabscesses).
Diagnosis of the disease is based on the clinical symptoms and complaints of the patient. Bimanual examination reveals infiltration and sharp pain of the affected area upon palpation; shortening the lateral layer of the vagina; displacement of the cervix to the side relative to the parametrium; the uterus is not palpable. A rectovaginal examination is mandatory to assess the degree of prolapse of the abscess into the rectum. Additionally, blood tests (clinical/biochemical), urinalysis, coagulogram, and kidney echography are performed. Diagnosis abroad is also carried out using ultrasound and CT.
Any treatment is prescribed only after consultation with the attending gynecologist and is comprehensive. The patient is prescribed antibacterial therapy, antifungal drugs, infusion therapy, desensitizing therapy, immunostimulating therapy, and correction of vaginal microflora is carried out. Treatment of postpartum parametritis in Israel involves surgical intervention in the event of the formation of a purulent abscess with a threat of breakthrough into nearby organs (bladder, rectum).
Prevention of the disease is the careful management of the birth process and the implementation of obstetric care; thorough postpartum diagnosis and care; maintaining personal hygiene.
Provided timely and adequate treatment, the prognosis for the life of patients with postpartum parametritis is favorable.
Parametritis - inflammation of the periuterine tissue - occurs with the lymphogenous spread of infection. The infection penetrates the tissue most often from ruptures of the cervix and upper third of the vagina, rarely from the placental area. Parametritis is predominantly one-sided. The exudate initially has a serous character, the amount of fibrin in it quickly increases, fibrin falls out, and a dense infiltrate forms. The inflammatory process may remain localized within the parametrium. Localization is facilitated by the loss of fibrin and the blockade of lymphatic pathways in the source of inflammation, the formation of a granulation shaft around it, and the presence of fibrous formations in the pelvic tissue, delimiting it into sections. In case of severe infection, these protective devices fail and the infection spreads to neighboring sections. Parametritis begins on the 10-12th day after birth with chills and fever up to 39°C, rarely up to 40°. The general condition of the postpartum mother suffers little, with complaints of mild nagging pain in the lower abdomen. Severe pain can appear at the very beginning of the disease - with irritation of the peritoneum covering the affected part of the tissue. At the very beginning of the disease, local symptoms are poorly expressed - vaginal examination reveals pastosity in the area of inflammation. After 2-3 days, the infiltrate is clearly contoured with a doughy and then dense consistency. The infiltrate is moderately painful and immobile. With parametritis, it is located between the lateral surface of the uterus and the pelvic wall, passing onto it with a wide wing. The lateral fornix becomes flattened and its mucous membrane loses mobility. The uterus cannot be palpated separately from the infiltrate and is displaced in the opposite direction in case of unilateral parametritis, and upward and anteriorly in case of bilateral parametritis. The infiltrate may extend beyond the parametrium. When it spreads anteriorly, it can be felt from the outside above the Pupart ligament. Due to the extraperitoneal location of the infiltrate, its upper palpation and upper percussion boundaries coincide; when percussing the upper anterior iliac spines on the affected side, a muted tone is obtained (Genter's symptom). When inflammation passes to the peri-vesical tissue, the infiltrate can spread along the posterior surface of the abdominal wall, taking the shape of a triangle with the apex facing the navel; the abdominal wall gives the impression of a starched shirtfront. From the upper part of the parametrium, the infiltrate can move behind the peritoneum up to the renal region. When the infiltrate is localized on the surface of the lumbar muscle (parapsoitis), the patient assumes a supine position with the leg abducted and bent. The course of parametritis varies. The febrile period (with slight remissions of temperature) lasts 1-2 weeks. The infiltrate gradually resolves. Suppuration is observed relatively rarely (at the 3-4th week of the disease). The temperature becomes remitting, and attacks of chills appear. If the abscess is not opened in a timely manner, the pus makes its way above the Poupart's ligament, through the sciatic foramen between the vessels on the buttock, under the Poupart's ligament on the thigh, and into the perinephric region. At the site of a threatening breakthrough of the abscess, a protrusion is first noted, and then redness of the skin and fluctuation. The abscess may also rupture into the bladder or rectum. With a threatening breakthrough in the bladder, tenesmus occurs, in the rectum - tension, diarrhea. Parametritis is distinguished as a separate form of the disease (primary parametritis) and as a reactive inflammation of the tissue in thrombophlebitis, adiexitis (secondary parametritis). Secondary parametritis is usually small in size. Currently, as a result of the use of antibiotics, primary parametritis is rare and usually mild. However, even during treatment with antibiotics, the possibility of transition to suppuration is not excluded, and its clinical picture may be erased.

Dream interpretation is an ancient art that allows you to at least assess the psychological status of a person, because...

As soon as the first mirrors were born, people immediately endowed them with all sorts of mystical abilities....

Photo: Anatoly ZHDANOV Understanding the program “The East is a delicate matter” on Radio “Komsomolskaya Pravda” [audio] Juma:...

Interpretation of the dream in the dream book: A man sees how he is being released from prison - the criminal sees great difficulties in life...

Making a new friend in a dream foreshadows the birth of a child. Seeing friends who have been absent for a long time - for the upcoming...

In the context of the implementation of the Federal State Educational Standard, it is of great importance. Over the course of decades, educational institutions have developed a system of work...

The manual discusses programs of domestic and foreign authors that are used in the work...

How often do we see this monster with goat horns when we lay out Tarot cards. "Devil" is the personification of hell...

Navigation: Description and history of the map: To the side of the road there is a large oak tree, in its foliage they find both shelter and food...
Dear forum visitors, I am opening this topic for fans of Patrick Walesa's "Deviant Tarot" deck...
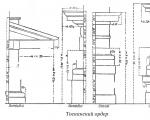
Tuscan order. Tuscan order, one of the five Roman architectural orders. The name is associated with...

LIBRETTO. If you love music (which you undoubtedly do, since you needed this book), then you'll probably...

Religion: paganism Birth: 942 (0942) Death: March on the Dnieper Family: Rurikovich Father:...

Masaccio (actually Tommaso di Giovanni di Simone Cassai (Guidi), Tommaso di ser Giovanni di Guidi; December 21...

As soon as the first mirrors were born, people immediately endowed them with all sorts of mystical abilities....

Photo: Anatoly ZHDANOV We understand the program “The East is a delicate matter” on Radio “Komsomolskaya Pravda” [audio]...