Philosophical vision of the problem
The meaning of life is related to the question “What to live for”, and not to the question of how to maintain life. A person's attitude is...
Principles of infusion rehydration therapy
General rules drawing up an infusion therapy program
1. Colloidal solutions contain sodium salts and belong to saline solutions and their volume must be taken into account in the total volume of saline solutions.
2. In total, colloidal solutions should not exceed 1/3 of the total daily volume of fluid for infusion therapy.
3. In young children, the ratio of glucose and salt solutions is 2:1 or 1:1; in older age, the amount of saline solutions increases (1:1 or 1:2).
3.1. The type of dehydration affects the ratio of glucose-saline solutions in the composition of infusion media.
4. All solutions must be divided into portions (“droppers”), the volume of which for glucose usually does not exceed 10-15 ml/kg and 7-10 ml for colloidal and saline solutions. The container for one drip should not contain more than ¼ of the daily volume of liquid. It is unrealistic to administer more than 3 drops per day to a child.
During infusion rehydration therapy, there are 4 stages: 1. anti-shock measures (1-3 hours); 2. Compensation for extracellular fluid deficiency (1-2-3 days); 3. maintaining water electrolyte balance in conditions of ongoing pathological losses (2-4 days or more); parenteral nutrition (total or partial) or therapeutic enteral nutrition.
To maintain a state of homeostasis, it is necessary to ensure a balance between the fluid introduced into the body and the fluid that the body removes in the form of urine, sweat, feces, and exhaled air. The amount and nature of losses varies depending on the nature of the disease.
The amount of fluid required to compensate for the physiological losses of the body in children of different ages is not the same.
Table 1. 69.Age-specific fluid and electrolyte requirements for children
The physiological need for sodium in young children is 3-5 mmol/kg; in older children, 2-3 mmol/kg;
The potassium requirement is 1-3 mmol/kg;
The requirement for magnesium is on average 0.1 mmol/kg.
The fluid and electrolyte requirements needed to replace physiological losses can be calculated using several methods.
Daily maintenance fluid (fluid requirement) can be calculated in several ways: 1) based on body surface area (there is a correlation between these indicators); 2) energy method (there is a relationship between energy needs and body weight). The minimum water requirement is 100-150 ml/100 kcal; 3) according to the Aberdeen nomogram (or tables made on its basis - table 1.69).
For some pathological conditions losses of water and/or electrolytes may increase or decrease significantly.
Table 1.70.Current pathological losses. Conditions that change fluid requirements
| State | Fluid requirement |
| Fever Hypothermia Uncontrollable vomiting Diarrhea Heart failure Pulmonary edema Increased sweating Hyperventilation Increased air humidity Renal failure Intestinal paresis Phototherapy High ambient temperature Increased metabolism Mechanical ventilation of newborns (with good hydration) | Increase by 10 ml/kg for each degree of increase in temperature Decrease by 10 ml/kg for each degree of decrease in temperature Increase in requirement by 20-30 ml/kg/day Increase by 25-50 ml/kg/day Reduction in requirement by 25-50% depending on the degree of deficiency Reducing the need to 20-30 ml/kg/day Increasing the need by 10-25 ml/100 kcal Increasing the need to 50-60 ml/100 kcal Reducing the need by 0-15 ml/100 kcal Reducing the need to 15 -30 ml/kg/day Increase in need by 25-50 ml/kg/day Increase in need by 15-30% Increase in need by 50-100% Increase in need by 25-75% Reduction in need by 20-30 ml/kg from daily requirement |
To cover the need for fluid, it is necessary to take into account the physiological need for fluid (1500-1800 ml/m 2) either calculated from tables (Table 1.69), or by the energy method and add to them the fluid losses identified in the patient.
General principles calculating the required fluid:
SZh = SZhP+ ZhVO+ZhVTPP, Where SJ– calculated daily fluid, SZhP– daily maintenance fluid, ZHVO– fluid to compensate for dehydration, ZhVCCI- liquid to compensate for current pathological losses.
Infusion therapy.
Infusion therapy– this is a drip or infusion intravenously or under the skin of drugs and biological fluids in order to normalize the water-electrolyte, acid-base balance of the body, as well as for forced diuresis (in combination with diuretics).
Indications to infusion therapy: all types of shock, blood loss, hypovolemia, loss of fluid, electrolytes and proteins as a result of uncontrollable vomiting, intense diarrhea, refusal to take fluids, burns, kidney disease; disturbances in the content of basic ions (sodium, potassium, chlorine, etc.), acidosis, alkalosis and poisoning.
Contraindications to infusion therapy are acute cardiovascular failure, pulmonary edema and anuria.
Principles of infusion therapy
The degree of risk of infusion, as well as preparation for it, should be lower than the expected positive result from infusion therapy.
The infusion should always be aimed at positive results. As a last resort, it should not aggravate the patient's condition.
Constant monitoring of the condition of both the patient and all indicators of the body’s functioning is required during the infusion.
Prevention of complications from the infusion procedure itself: thrombophlebitis, disseminated intravascular coagulation, sepsis, hypothermia.
Goals of infusion therapy: restoration of blood volume, elimination of hypovolemia, ensuring adequate cardiac output, maintaining and restoring normal plasma osmolarity, ensuring adequate microcirculation, preventing aggregation shaped elements blood, normalization of the oxygen transport function of the blood.
There are basic and corrective I. t. The purpose of basic I. t. is to provide the body with physiological needs for water or electrolytes. Corrective I. is aimed at correcting changes in water, electrolyte, protein balance and blood by replenishing missing volume components (extracellular and cellular fluid), normalizing the disturbed composition and osmolarity of water spaces, hemoglobin levels and plasma colloid osmotic pressure.
Infusion solutions are divided into crystalloid and colloid. TO crystalloid include solutions of sugars (glucose, fructose) and electrolytes. They can be isotonic, hypotonic and hypertonic in relation to the value of normal plasma osmolarity. Sugar solutions are the main source of free (electrolyte-free) water, and therefore they are used for maintenance hydration therapy and to correct free water deficiency. The minimum physiological need for water is 1200 ml/day Electrolyte solutions (physiological, Ringer's, Ringer-Locke, lactasol, etc.) are used to compensate for electrolyte losses. The ionic composition of physiological solution, Ringer's, Ringer-Locke solutions does not correspond to the ionic composition of plasma, since the main ions in them are sodium and chlorine ions, and the concentration of the latter significantly exceeds its concentration in plasma. Electrolyte solutions are indicated in cases of acute loss of extracellular fluid, consisting predominantly of these ions. The average daily sodium requirement is 85 mEq/m 2 and can be fully provided with electrolyte solutions. Daily potassium requirement (51 mEq/m 2 ) replenish polarizing potassium mixtures with glucose solutions and insulin. Use 0.89% sodium chloride solution, Ringer and Ringer-Locke solutions, 5% sodium chloride solution, 5-40% glucose solutions and other solutions. They are administered intravenously and subcutaneously, in a stream (in case of severe dehydration) and drip, in a volume of 10–50 or more ml/kg. These solutions do not cause complications, except for overdose.
Solution (0.89%) sodium chloride is isotonic with human blood plasma and therefore quickly cleared from the vascular bed, only temporarily increasing the volume of circulating fluid, so its effectiveness in cases of blood loss and shock is insufficient. Hypertonic solutions (3-5-10%) are used intravenously and externally. When applied externally, they promote the secretion of pus, exhibit antimicrobial activity, and when administered intravenously, they increase diuresis and replenish the deficiency of sodium and chlorine ions.
Ringer's solution- multicomponent physiological solution. A solution in distilled water of several inorganic salts with precisely maintained concentrations, such as sodium chloride, potassium chloride, calcium chloride, as well as sodium bicarbonate to stabilize the acidity of the solution pH as a buffer component. Administered intravenously in a dose of 500 to 1000 ml/day. The total daily dose is up to 2-6% of body weight.
Glucose solutions. Isotonic solution (5%) - subcutaneously, 300–500 ml; IV (drip) - 300–2000 ml/day. Hypertonic solutions (10% and 20%) - intravenously, once - 10–50 ml or drip up to 300 ml/day.
Ascorbic acid solution for injection. IV - 1 ml of 10% or 1–3 ml of 5% solution. Highest dose: single - not higher than 200 mg, daily - 500 mg.
To compensate for the loss of isotonic fluid (for burns, peritonitis, intestinal obstruction, septic and hypovolemic shock), solutions with an electrolyte composition close to plasma (lactasol, ringer-lactate solution) are used. With a sharp decrease in plasma osmolarity (below 250 mOsm/l) hypertonic (3%) sodium chloride solutions are used. When plasma sodium concentration increases to 130 mmol/l the administration of hypertonic solutions of sodium chloride is stopped and isotonic solutions are prescribed (lactasol, ringer lactate and saline s). When plasma osmolarity increases due to hypernatremia, solutions are used that reduce plasma osmolarity: first 2.5% and 5% glucose solutions, then hypotonic and isotonic solutions of electrolytes with glucose solutions in a 1:1 ratio.
Colloidal solutions- These are solutions of high molecular weight substances. They help retain fluid in the vascular bed. These include dextrans, gelatin, starch, as well as albumin, protein, and plasma. They use hemodez, polyglucin, reopoliglucin, reogluman. Colloids have a higher molecular weight than crystalloids, which ensures their longer stay in the vascular bed. Colloidal solutions restore plasma volume faster than crystalloid ones, which is why they are called plasma substitutes. In terms of their hemodynamic effect, solutions of dextran and starch are significantly superior to crystalloid solutions. To obtain an antishock effect, a significantly smaller amount of these media is required compared to solutions of glucose or electrolytes. With loss of fluid volume, especially with blood and plasma loss, these solutions quickly increase venous flow to the heart, filling of the heart cavities, cardiac output and stabilize blood pressure. However, colloid solutions can cause circulatory overload more quickly than crystalloid solutions. Routes of administration: intravenous, less often subcutaneous and drip. The total daily dose of zadextrans should not exceed 1.5-2 g/kg due to the risk of bleeding that may occur as a result of blood coagulation disorders. Renal dysfunction (dextran kidney) and anaphylactic reactions are sometimes observed. They have detoxifying properties. They are used as a source of parenteral nutrition in cases of prolonged refusal to eat or inability to feed by mouth. Blood and casein hydrolysins are used (Alvesin-Neo, polyamine, lipofundin, etc.). They contain amino acids, lipids and glucose.
In cases of acute hypovolemia and shock, colloidal solutions are used as media that quickly restore intravascular volume. In hemorrhagic shock initial stage treatment to quickly restore circulating blood volume (CBV) use polyglucin or any other dextran with a molecular weight of 60,000-70,000, which are transfused very quickly in a volume of up to 1 l. The rest of the lost blood volume is replaced with solutions of gelatin, plasma and blood. Part of the lost blood volume is compensated by administering isotonic electrolyte solutions, preferably a balanced composition in proportion to the lost volume as 3:1 or 4:1. In case of shock associated with loss of fluid volume, it is necessary not only to restore bcc, but also to fully satisfy the body's needs for water and electrolytes. Albumin is used to correct plasma protein levels.
The main thing in the treatment of fluid deficiency in the absence of blood loss or osmolarity disorders is the replacement of this volume with balanced salt solutions. For moderate fluid deficiency, isotonic electrolyte solutions are prescribed (2.5-3.5 l/day). With severe fluid loss, the volume of infusions should be significantly larger.
Volume of infused liquid. There is a simple formula proposed by L. Denis (1962):
with 1st degree dehydration (up to 5%) - 130-170 ml/kg/24h;
2nd degree (5-10%) - 170-200 ml/kg/24 hours;
3rd degree (> 10%) - 200-220 ml/kg/24 hours.
Calculation of the total volume of infusate per day is carried out as follows: an amount of liquid equal to the decrease in weight (water deficiency) is added to the age-related physiological requirement. Additionally, 30-60 ml is added for each kg of body weight to cover current losses. With hyperthermia and high temperature environment, add 10 ml of infusate for each degree of body temperature exceeding 37°. 75-80% of the total volume of the calculated fluid is administered intravenously, the rest is given in the form of drink.
Calculation of the volume of daily infusion therapy: Universal method:(For all types of dehydration).
Volume = daily requirement + pathological losses + deficiency.
Daily requirement - 20-30 ml/kg; at ambient temperature more than 20 degrees
For each degree +1 ml/kg.
Pathological losses:
Vomiting - approximately 20-30 ml/kg (it is better to measure the volume of losses);
Diarrhea - 20-40 ml/kg (it is better to measure the volume of losses);
Intestinal paresis - 20-40 ml/kg;
Temperature - +1 degree = +10ml/kg;
RR more than 20 per minute - + 1 breath = +1ml/kg ;
Volume of discharge from drainage, probe, etc.;
Polyuria - diuresis exceeds the individual daily requirement.
Dehydration: 1. Skin elasticity or turgor; 2. Contents of the bladder; 3. Body weight.
Physiological examination: skin elasticity or turgor is an approximate measure of dehydration:< 5% ВТ - не определяется;
5-6% - skin turgor is slightly reduced;
6-8% - skin turgor is noticeably reduced;
10-12% - the skin fold remains in place;
Metrogyl solution. Ingredients: metronidazole, sodium chloride, lemon acid(monohydrate), sodium hydrogen phosphate anhydrous, water d/i. Antiprotozoal and antimicrobial drug, a derivative of 5-nitroimidazole. IV administration of the drug is indicated for severe infections, as well as in the absence of the possibility of taking the drug orally.
Adults and children over 12 years old - at an initial dose of 0.5-1 g intravenously (duration of infusions - 30-40 minutes), and then every 8 hours, 500 mg at a rate of 5 ml/min. If well tolerated, after the first 2-3 infusions they switch to jet administration. The course of treatment is 7 days. If necessary, intravenous administration is continued for a longer time. The maximum daily dose is 4 g. According to indications, switch to maintenance oral administration at a dose of 400 mg 3 times a day.
To hemostatic drugs include cryoprecipitate, prothrombin complex, fibrinogen. The cryoprecipitate contains large amounts of antihemophilic globulin (blood coagulation factor VIII) and von Willebrand factor, as well as fibrinogen, fibrin-stabilizing factor XIII and impurities of other proteins. The drugs are released in plastic bags or bottles in frozen or dried form. Fibrinogen has limited use: it is indicated for bleeding caused by fibrinogen deficiency.
 Infusion therapy healing method, consisting in the parenteral introduction into the patient’s body of the necessary components of vital activity, distributed in the aqueous phase. Infusion-transfusion therapy (Isakov Yu. F., Mikhelson V. A., Shtatnov M. K. 1985)
Infusion therapy healing method, consisting in the parenteral introduction into the patient’s body of the necessary components of vital activity, distributed in the aqueous phase. Infusion-transfusion therapy (Isakov Yu. F., Mikhelson V. A., Shtatnov M. K. 1985)
 Indications for infusion therapy Reimbursement of blood volume Improvement of tissue perfusion Reimbursement of fluid deficiency during dehydration Maintaining physiological needs Reimbursement of losses (bleeding, burns, diarrhea) Forced diuresis during exotoxicosis Support during surgery Transfusion of blood components Nutritional support (TPN, PPN) (Mensach IVECCS, 2005)
Indications for infusion therapy Reimbursement of blood volume Improvement of tissue perfusion Reimbursement of fluid deficiency during dehydration Maintaining physiological needs Reimbursement of losses (bleeding, burns, diarrhea) Forced diuresis during exotoxicosis Support during surgery Transfusion of blood components Nutritional support (TPN, PPN) (Mensach IVECCS, 2005)
 - transfusion therapy - transfusion of blood products - infusion therapy - administration of simple and complex solutions, synthetic drugs, emulsions and PP preparations
- transfusion therapy - transfusion of blood products - infusion therapy - administration of simple and complex solutions, synthetic drugs, emulsions and PP preparations
 Processes that determine approaches to infusion therapy (Isakov Yu. F., Mikhelson V. A., Shtatnov M. K., 1985) Water content in the body as a whole Characteristics of the body’s water spaces State of exchange of water and electrolytes between the body and external environment State of interdimensional water exchange
Processes that determine approaches to infusion therapy (Isakov Yu. F., Mikhelson V. A., Shtatnov M. K., 1985) Water content in the body as a whole Characteristics of the body’s water spaces State of exchange of water and electrolytes between the body and external environment State of interdimensional water exchange
 Water spaces of the body (classification by J. S. Edelman, J. Leibman 1959) Intracellular fluid (space) Extracellular fluid (space) ï intravascular ï intercellular fluid (actually interstitial) ï transcellular fluid - water in the secretions of the gastrointestinal tract, digestive and other glands, urine, cerebrospinal fluid, eye cavity fluid, discharge serous membranes, synovial fluid Infusion therapy and parenteral nutrition
Water spaces of the body (classification by J. S. Edelman, J. Leibman 1959) Intracellular fluid (space) Extracellular fluid (space) ï intravascular ï intercellular fluid (actually interstitial) ï transcellular fluid - water in the secretions of the gastrointestinal tract, digestive and other glands, urine, cerebrospinal fluid, eye cavity fluid, discharge serous membranes, synovial fluid Infusion therapy and parenteral nutrition
 Third space An abstract sector in which fluid is sequestered from both the extracellular and intracellular spaces. Temporarily the fluid of this space is not available for exchange, which leads to clinical manifestations liquid shortages in relevant sectors
Third space An abstract sector in which fluid is sequestered from both the extracellular and intracellular spaces. Temporarily the fluid of this space is not available for exchange, which leads to clinical manifestations liquid shortages in relevant sectors
 Third space Intestinal contents with intestinal paresis Edema fluid with ascites, exudate with peritonitis Soft tissue swelling with a burn Traumatic surgical interventions (evaporation from the surface)
Third space Intestinal contents with intestinal paresis Edema fluid with ascites, exudate with peritonitis Soft tissue swelling with a burn Traumatic surgical interventions (evaporation from the surface)
 Third space The volume of the third space cannot be reduced by limiting the administration of fluids and salts. On the contrary, to maintain an adequate level of hydrobalance (intracellular and extracellular fluid), infusion is required in a volume exceeding the physiological need
Third space The volume of the third space cannot be reduced by limiting the administration of fluids and salts. On the contrary, to maintain an adequate level of hydrobalance (intracellular and extracellular fluid), infusion is required in a volume exceeding the physiological need
 TYPES OF SEMI-PERMEABLE MEMBRANES The fluid sectors of the body are separated from each other by a selectively permeable membrane through which water and some substrates dissolved in it move. 1. Cell membranes, which are composed of lipids and proteins and separate intracellular and interstitial fluid. 2. Capillary membranes separate intravascular fluid from transcellular fluid. 3. Epithelial membranes, which are the epithelium of the mucous membranes of the stomach, intestines, synovial membranes and renal tubules. Epithelial membranes separate interstitial and intravascular fluid from transcellular fluid.
TYPES OF SEMI-PERMEABLE MEMBRANES The fluid sectors of the body are separated from each other by a selectively permeable membrane through which water and some substrates dissolved in it move. 1. Cell membranes, which are composed of lipids and proteins and separate intracellular and interstitial fluid. 2. Capillary membranes separate intravascular fluid from transcellular fluid. 3. Epithelial membranes, which are the epithelium of the mucous membranes of the stomach, intestines, synovial membranes and renal tubules. Epithelial membranes separate interstitial and intravascular fluid from transcellular fluid.
 Changes in the water content in the body depending on age (Friis., 1957, Groer M.W. 1981) Age The proportion of fluid in body weight, % Premature. newborn 80 Full-term newborn 1 -10 days 1 -3 months 6 -12 months 1 -2 years 2 -3 years 3 -5 years 5 -10 years 10 -16 years 75 74 79, 3 70 60 60, 4 58, 7 63 5 62, 2 61, 5 58
Changes in the water content in the body depending on age (Friis., 1957, Groer M.W. 1981) Age The proportion of fluid in body weight, % Premature. newborn 80 Full-term newborn 1 -10 days 1 -3 months 6 -12 months 1 -2 years 2 -3 years 3 -5 years 5 -10 years 10 -16 years 75 74 79, 3 70 60 60, 4 58, 7 63 5 62, 2 61, 5 58
 Relative values of water content in the extra- and intracellular space in children of different ages (Friis N.V., 1951) age 0 -1 day 1 -10 days 1 -3 months 3 -6 months 6 -12 months 1 -2 years 2 - 3 years 3 -5 years 5 -10 years 10 -16 years ECF content, % 43, 9 39, 7 32, 2 30, 1 27, 4 25, 6 25. 7 21, 4 22 18. 7 ICF content, % 35, 1 34, 4 40, 1 40 33 33, 1 36, 8 40, 8 39 39, 3
Relative values of water content in the extra- and intracellular space in children of different ages (Friis N.V., 1951) age 0 -1 day 1 -10 days 1 -3 months 3 -6 months 6 -12 months 1 -2 years 2 - 3 years 3 -5 years 5 -10 years 10 -16 years ECF content, % 43, 9 39, 7 32, 2 30, 1 27, 4 25, 6 25. 7 21, 4 22 18. 7 ICF content, % 35, 1 34, 4 40, 1 40 33 33, 1 36, 8 40, 8 39 39, 3
 Physiology of water balance Osmolality - the number of osmotically active particles in 1000 g of water in solution (unit of measurement - mOsm/kg) Osmolarity - the number of osmotically active particles per unit volume of solution (unit of measurement - mOsm/l) Infusion therapy and parenteral nutrition
Physiology of water balance Osmolality - the number of osmotically active particles in 1000 g of water in solution (unit of measurement - mOsm/kg) Osmolarity - the number of osmotically active particles per unit volume of solution (unit of measurement - mOsm/l) Infusion therapy and parenteral nutrition
 PLASMA OSMOLALITY True normoosmia - 285 ± 5 mOsm/kg H 2 O Compensated normoosmolality - from 280 to 310 mOsm/kg H 2 O Colloid-oncotic pressure from 18 to 25 mm. rt. Art.
PLASMA OSMOLALITY True normoosmia - 285 ± 5 mOsm/kg H 2 O Compensated normoosmolality - from 280 to 310 mOsm/kg H 2 O Colloid-oncotic pressure from 18 to 25 mm. rt. Art.

 Hydration and osmolarity disorders: GENERAL RULES Everything always starts with the extracellular sector! It also determines the type of osmolarity disorder. It also determines the overall fluid balance. He is the leader, and the cell is the slave sector! Osmolarity inside the cell is considered normal! Osmolarity losses are the opposite of the total! Water moves towards higher osmolarity. Dehydration does not exclude edema!
Hydration and osmolarity disorders: GENERAL RULES Everything always starts with the extracellular sector! It also determines the type of osmolarity disorder. It also determines the overall fluid balance. He is the leader, and the cell is the slave sector! Osmolarity inside the cell is considered normal! Osmolarity losses are the opposite of the total! Water moves towards higher osmolarity. Dehydration does not exclude edema!
 Intravenous fluid requirement in children 20 kg 1500 ml + (20 ml/kg for each kg over 20 kg) Weight 10 12 14 1 6 18 20 30 35 40 50 60 70 ml/h ac 40 45 50 5 5 60 65 70 75 80 90 95 100
Intravenous fluid requirement in children 20 kg 1500 ml + (20 ml/kg for each kg over 20 kg) Weight 10 12 14 1 6 18 20 30 35 40 50 60 70 ml/h ac 40 45 50 5 5 60 65 70 75 80 90 95 100
 Fluid requirement in children 0 -10 kg = 4 ml/kg/hour 11 -20 kg = 40 ml/hour + 2 ml/kg/over 10 20 -40 kg = 60 ml/hour +1 ml/kg/over 20 FP (ml/kg/day) = 100 – (3*age (year) Vallachi formula
Fluid requirement in children 0 -10 kg = 4 ml/kg/hour 11 -20 kg = 40 ml/hour + 2 ml/kg/over 10 20 -40 kg = 60 ml/hour +1 ml/kg/over 20 FP (ml/kg/day) = 100 – (3*age (year) Vallachi formula
 Choice of vascular access Peripheral veins – infusion requirement 1-3 days; no need to administer hyperosmolar solutions Central vein – the need for infusion for 3 days or more; Parenteral nutrition; Administration of hyperosmolar solutions Intraosseous needle - Antishock therapy
Choice of vascular access Peripheral veins – infusion requirement 1-3 days; no need to administer hyperosmolar solutions Central vein – the need for infusion for 3 days or more; Parenteral nutrition; Administration of hyperosmolar solutions Intraosseous needle - Antishock therapy

 Emergency fluid replacement Ø In the 1st phase of volume resuscitation, a bolus of saline Na solution is performed. Cl or Ringer's Lactate In a volume of 10 -20 ml/kg over 30 minutes Ø A repeated bolus of fluid may be required until hemodynamic stabilization
Emergency fluid replacement Ø In the 1st phase of volume resuscitation, a bolus of saline Na solution is performed. Cl or Ringer's Lactate In a volume of 10 -20 ml/kg over 30 minutes Ø A repeated bolus of fluid may be required until hemodynamic stabilization
 Albumin vs Phys. solution There are no significant differences: Mortality Time of hospitalization in the intensive care unit Time of hospitalization in the hospital Duration of mechanical ventilation Therefore... we use crystalloids
Albumin vs Phys. solution There are no significant differences: Mortality Time of hospitalization in the intensive care unit Time of hospitalization in the hospital Duration of mechanical ventilation Therefore... we use crystalloids
 How big is the deficit? Fluid deficit = weight before illness (kg) - actual weight % dehydration = (weight before illness - actual weight) weight before illness x 100%
How big is the deficit? Fluid deficit = weight before illness (kg) - actual weight % dehydration = (weight before illness - actual weight) weight before illness x 100%
 signs Loss of body weight (%) Liquid deficiency. (ml/kg) Vital signs Pulse BP Breathing Children under 1 year Skin - color - cold - capillary refill (sec) Over 1 year mild 5 50 moderate 10 100 severe 15 150 N N N Thirst, restlessness, anxiety rapid From N to low Deep To same, or lethargy Very frequent, threads. Shock Deep and frequent Drowsiness to the point of coma, lethargy, sweating. pale Down from the middle of the forearm/shin 3 -4 grayish From the middle of the forearm/thigh 4 -5 spotted Entire limb Same as above Usually coma, cyanosis 5 Skin turgor Anterior fontanelle N N Same, and postural hypertension reduced Sunken Eyeballs N Sunken Tears Yes +/- Significantly reduced Significantly sunken Significantly sunken Absent Mucous under the armpit Urine Diuresis (ml/kg/hour) Spec. density Acidosis Wet Yes Dry no Very dry no ↓ 2 1,020 - ↓ 1 1.020 -1,030 +/- ↓ 0.5 1,030 + Increased blood urea nitrogen - + ++
signs Loss of body weight (%) Liquid deficiency. (ml/kg) Vital signs Pulse BP Breathing Children under 1 year Skin - color - cold - capillary refill (sec) Over 1 year mild 5 50 moderate 10 100 severe 15 150 N N N Thirst, restlessness, anxiety rapid From N to low Deep To same, or lethargy Very frequent, threads. Shock Deep and frequent Drowsiness to the point of coma, lethargy, sweating. pale Down from the middle of the forearm/shin 3 -4 grayish From the middle of the forearm/thigh 4 -5 spotted Entire limb Same as above Usually coma, cyanosis 5 Skin turgor Anterior fontanelle N N Same, and postural hypertension reduced Sunken Eyeballs N Sunken Tears Yes +/- Significantly reduced Significantly sunken Significantly sunken Absent Mucous under the armpit Urine Diuresis (ml/kg/hour) Spec. density Acidosis Wet Yes Dry no Very dry no ↓ 2 1,020 - ↓ 1 1.020 -1,030 +/- ↓ 0.5 1,030 + Increased blood urea nitrogen - + ++
 Calculation of infusion for 24 hours 1 -8 hours - 50% of the calculated volume 8 -24 hours - 50% of the calculated volume Resuscitation fluid is not included in the total volume
Calculation of infusion for 24 hours 1 -8 hours - 50% of the calculated volume 8 -24 hours - 50% of the calculated volume Resuscitation fluid is not included in the total volume
 signs Iso Hyper Serum Na (mol/l) 130 -150 ↓ 130 150 and N Osmolarity N ↓N N Avg. Volume er. (MCV)N N N or ↓N Average in er-ts. (MSN)N ↓N N Consciousness Lethargy Coma/convulsions. Thirst Moderate Weak Excitability/judgment Strong Skin turgor Poor Adequate Palpable skin Dry Very poor Sticky Skin temperature N Low Increased Mucous membranes Dry Sticky Tachycardia ++ ++ + Hypotension ++ + Oligouria ++ + History Loss through the gastrointestinal tract and kidneys, blood loss, plasma loss. Deficiency or loss of salts Deficiency or loss of water Dense doughy
signs Iso Hyper Serum Na (mol/l) 130 -150 ↓ 130 150 and N Osmolarity N ↓N N Avg. Volume er. (MCV)N N N or ↓N Average in er-ts. (MSN)N ↓N N Consciousness Lethargy Coma/convulsions. Thirst Moderate Weak Excitability/judgment Strong Skin turgor Poor Adequate Palpable skin Dry Very poor Sticky Skin temperature N Low Increased Mucous membranes Dry Sticky Tachycardia ++ ++ + Hypotension ++ + Oligouria ++ + History Loss through the gastrointestinal tract and kidneys, blood loss, plasma loss. Deficiency or loss of salts Deficiency or loss of water Dense doughy
 Is hematocrit relevant? Yes! For isotonic disorders No! For hypo or hypertensive disorders
Is hematocrit relevant? Yes! For isotonic disorders No! For hypo or hypertensive disorders

 Isoosmolar dehydration Calculation of fluid deficiency: Eliminating the cause! Volume replacement with isotonic media (Na.Cl 0.9%, Sterofundin) Control by Ht is possible
Isoosmolar dehydration Calculation of fluid deficiency: Eliminating the cause! Volume replacement with isotonic media (Na.Cl 0.9%, Sterofundin) Control by Ht is possible


 Hyperosmolar dehydration Water deficiency Hyperventilation Profuse sweating Hypo- or isosthenuria Risk of damage to the central nervous system (rupture of perforating veins, subdural hematoma)
Hyperosmolar dehydration Water deficiency Hyperventilation Profuse sweating Hypo- or isosthenuria Risk of damage to the central nervous system (rupture of perforating veins, subdural hematoma)
 Hyperosmolar dehydration Calculation of free water deficiency is inaccurate: Elimination of the cause! Replenish the deficiency with 0.45% Na. Cl or 5% glucose “Titration” of the effect is necessary!
Hyperosmolar dehydration Calculation of free water deficiency is inaccurate: Elimination of the cause! Replenish the deficiency with 0.45% Na. Cl or 5% glucose “Titration” of the effect is necessary!
 Hyperosmolar dehydration Starting solution Ringer-Lactate / saline. solution Monitor Na level every 2-4 hours – Proper rate of Na reduction 0.5 -1 mmol/l/hour (10 mmol/l/day) – Do not reduce more than 15 mmol/l/day If Na is not corrected: – Go to ratio 5% glucose/physical. solution 1/4 Sodium is not corrected – Calculation of total body water deficit (TBWD) TBWD = 4 ml/kg x weight x (patient’s sodium - 145) – Reimbursement of fluid deficiency within 48 hours Glucose 5%/sodium chloride 0.9% 1 /2
Hyperosmolar dehydration Starting solution Ringer-Lactate / saline. solution Monitor Na level every 2-4 hours – Proper rate of Na reduction 0.5 -1 mmol/l/hour (10 mmol/l/day) – Do not reduce more than 15 mmol/l/day If Na is not corrected: – Go to ratio 5% glucose/physical. solution 1/4 Sodium is not corrected – Calculation of total body water deficit (TBWD) TBWD = 4 ml/kg x weight x (patient’s sodium - 145) – Reimbursement of fluid deficiency within 48 hours Glucose 5%/sodium chloride 0.9% 1 /2



 Hypoosmolar dehydration Calculation of Na+ deficiency is unreliable: Elimination of the cause! Replenishment of Na+ deficiency 5.85% or 7.2% Na. Cl + KCl Caution: pontine myelinolysis! Monitor Na every 2 hours. The rate of increase in Na is not more than 2 mmol/l/hour
Hypoosmolar dehydration Calculation of Na+ deficiency is unreliable: Elimination of the cause! Replenishment of Na+ deficiency 5.85% or 7.2% Na. Cl + KCl Caution: pontine myelinolysis! Monitor Na every 2 hours. The rate of increase in Na is not more than 2 mmol/l/hour
 Hyponatremic seizures Increase sodium level by 5 mmol/l by administering 6 ml/kg 3% Na. Cl – Inject 3% Na. Cl (0.5 mEq Na.Cl/ml) IV over 1 hour – Administer 3% Na. Cl at a rate of 6 ml/kg/hour until the seizures are relieved. Seizures occur as a result of cerebral edema. It is possible to use Na. HCO 3 8% 1 ml/kg
Hyponatremic seizures Increase sodium level by 5 mmol/l by administering 6 ml/kg 3% Na. Cl – Inject 3% Na. Cl (0.5 mEq Na.Cl/ml) IV over 1 hour – Administer 3% Na. Cl at a rate of 6 ml/kg/hour until the seizures are relieved. Seizures occur as a result of cerebral edema. It is possible to use Na. HCO 3 8% 1 ml/kg
 Hypoosmolar overhydration Heart failure Excess hypotonic solutions Pain (via ADH) Syndrome of inappropriate ADH secretion (SIADH)
Hypoosmolar overhydration Heart failure Excess hypotonic solutions Pain (via ADH) Syndrome of inappropriate ADH secretion (SIADH)

 Composition of infusion therapy -Izoosmolar dehydration with glucose-salt in a ratio of 1/1 -1/2 -Hypo-osmolar dehydration with glucose-salt in a ratio of 1/2-1/4 (up to some saline solutions) -Hyperosmolar dehydration with glucose-salt in a ratio of 2: 1 (up to the infusion of one 5 -10% Glucose under sugar control, with the possible use of insulin
Composition of infusion therapy -Izoosmolar dehydration with glucose-salt in a ratio of 1/1 -1/2 -Hypo-osmolar dehydration with glucose-salt in a ratio of 1/2-1/4 (up to some saline solutions) -Hyperosmolar dehydration with glucose-salt in a ratio of 2: 1 (up to the infusion of one 5 -10% Glucose under sugar control, with the possible use of insulin

 Fluid Load Mode (FLR) FLR = FP + PP FLR is the primary rehydration regimen in most cases. Pathological losses (PP) 1. Obvious losses are measured by compensation. 1: 1 (vomiting, discharge through a tube, stool, etc.) 2. Fever +10 ml/kg/day for every degree 10 above normal. 3. Shortness of breath +10 ml/kg/day for every 10 breaths. above normal! 4. Paresis 1st degree. -10 ml/kg/day. 2 tbsp. -20 ml/kg/day; 3 tbsp. -30 ml/kg/day. 5. Phototherapy 10 ml/kg/day.
Fluid Load Mode (FLR) FLR = FP + PP FLR is the primary rehydration regimen in most cases. Pathological losses (PP) 1. Obvious losses are measured by compensation. 1: 1 (vomiting, discharge through a tube, stool, etc.) 2. Fever +10 ml/kg/day for every degree 10 above normal. 3. Shortness of breath +10 ml/kg/day for every 10 breaths. above normal! 4. Paresis 1st degree. -10 ml/kg/day. 2 tbsp. -20 ml/kg/day; 3 tbsp. -30 ml/kg/day. 5. Phototherapy 10 ml/kg/day.
 Fluid loading regime (LNG) Volume of infusion therapy according to the degree of dehydration (Denis’s table) age I degree III wall 0 – 3 months 200 ml/kg 220 -240 ml/kg 250 -300 ml/kg 3 – 6 months 170 -180 200 - 220 220 -250 6 – 12 months 150 -170 170 -200 200 -220 1 – 3 years 130 -150 Up to 170 Up to 200 3 – 5 years 110 -130 Up to 150 Up to 180
Fluid loading regime (LNG) Volume of infusion therapy according to the degree of dehydration (Denis’s table) age I degree III wall 0 – 3 months 200 ml/kg 220 -240 ml/kg 250 -300 ml/kg 3 – 6 months 170 -180 200 - 220 220 -250 6 – 12 months 150 -170 170 -200 200 -220 1 – 3 years 130 -150 Up to 170 Up to 200 3 – 5 years 110 -130 Up to 150 Up to 180
 Fluid load mode (RLG) RGG = 1.7 FP + PP 1.7 FP = 1.0 FP+ 0.7 daily diuresis (on average 70% of FP) Indications - toxicosis of various origins Contraindications to RGG - Age up to 1 year (high tissue hydrophilicity, immaturity of systems for removing excess fluid) - Renal and postrenal acute renal failure - Prerenal cardiogenic acute renal failure - Heart failure - Cerebral edema
Fluid load mode (RLG) RGG = 1.7 FP + PP 1.7 FP = 1.0 FP+ 0.7 daily diuresis (on average 70% of FP) Indications - toxicosis of various origins Contraindications to RGG - Age up to 1 year (high tissue hydrophilicity, immaturity of systems for removing excess fluid) - Renal and postrenal acute renal failure - Prerenal cardiogenic acute renal failure - Heart failure - Cerebral edema
 Liquid load mode (RLG) Hyperhydration mode with acute poisoning Mild degree- if possible, enteral load, enterosorption. If it is not possible, the method of forced diuresis (FD) = 7.5 ml/kg/hour for no more than 4 hours with a transition to physical. need. Moderate degree - PD = 10 -15 ml/kg/hour Severe degree - PD = 15 -20 ml/kg/hour Composition: polyionic solutions, saline. solution, Ringer solution, 10% glucose solution
Liquid load mode (RLG) Hyperhydration mode with acute poisoning Mild degree- if possible, enteral load, enterosorption. If it is not possible, the method of forced diuresis (FD) = 7.5 ml/kg/hour for no more than 4 hours with a transition to physical. need. Moderate degree - PD = 10 -15 ml/kg/hour Severe degree - PD = 15 -20 ml/kg/hour Composition: polyionic solutions, saline. solution, Ringer solution, 10% glucose solution
 Fluid load mode (RDG) RDG = 2/3 – 1/3 of RNG Indications: -Heart failure (SSN-1 st. 2/3 from RNG; SSN-2 st. 1/2 from RNG; SSN-3 st. 1/3) - Cerebral edema (2/3 from RNG to the full volume of RNG with stabilization of hemodynamics to maintain ICP.) - Acute pneumonia, RDS (from 1/3 to 2/3 AF) - Renal, postrenal and cardiogenic prerenal acute renal failure (1/3 AF + diuresis correction every 6 -8 hours.)
Fluid load mode (RDG) RDG = 2/3 – 1/3 of RNG Indications: -Heart failure (SSN-1 st. 2/3 from RNG; SSN-2 st. 1/2 from RNG; SSN-3 st. 1/3) - Cerebral edema (2/3 from RNG to the full volume of RNG with stabilization of hemodynamics to maintain ICP.) - Acute pneumonia, RDS (from 1/3 to 2/3 AF) - Renal, postrenal and cardiogenic prerenal acute renal failure (1/3 AF + diuresis correction every 6 -8 hours.)
 Correction of protein-electrolyte and metabolic disorders Content of electrolytes in mmol preparations 1 g Na. Cl 1 g KCl 1 g Ca. Cl 2 1 g Mq. SO 4 Electrolyte content in mmol 17.2 mmol Na 13.4 mmol K 2.3 mol Ca 4.5 mmol Ca 4.0 mmol Mq Correction of decompensated met. acidosis. Volume of 4% soda (ml) = BE x weight/2 It is used only if the ability and function of breathing to compensate is preserved.
Correction of protein-electrolyte and metabolic disorders Content of electrolytes in mmol preparations 1 g Na. Cl 1 g KCl 1 g Ca. Cl 2 1 g Mq. SO 4 Electrolyte content in mmol 17.2 mmol Na 13.4 mmol K 2.3 mol Ca 4.5 mmol Ca 4.0 mmol Mq Correction of decompensated met. acidosis. Volume of 4% soda (ml) = BE x weight/2 It is used only if the ability and function of breathing to compensate is preserved.
 Perioperative Fluid Therapy Goal: Maintain fluid and electrolyte balance Correct hypovolemia Ensure adequate tissue perfusion
Perioperative Fluid Therapy Goal: Maintain fluid and electrolyte balance Correct hypovolemia Ensure adequate tissue perfusion

 Perioperative Fluid Therapy Pediatrics 1957 Recommended 5% glucose/0.2% Na. Cl for basic infusion therapy Based on the amount of human milk electrolytes
Perioperative Fluid Therapy Pediatrics 1957 Recommended 5% glucose/0.2% Na. Cl for basic infusion therapy Based on the amount of human milk electrolytes
 First publication – 16 healthy children – All underwent elective surgery – Severe Hyponatremia and Brain Edema death/permanent neurological impairment – All received Hypotonic Hyponatremic solution
First publication – 16 healthy children – All underwent elective surgery – Severe Hyponatremia and Brain Edema death/permanent neurological impairment – All received Hypotonic Hyponatremic solution

 . . . Oct. 1, 2006 The risk of developing hyponatremia after receiving hypotonic solutions is 17.2 times greater Prescribing hypotonic solutions is not reliable/harmful
. . . Oct. 1, 2006 The risk of developing hyponatremia after receiving hypotonic solutions is 17.2 times greater Prescribing hypotonic solutions is not reliable/harmful
 Perioperative fluid therapy National Guidelines 2007 (UK GOVERNMENT SAFETY AGENCY) 4% glucose solution and 0.18% sodium chloride solution should not be used in routine practice Intra- and postoperatively use only isotonic solutions
Perioperative fluid therapy National Guidelines 2007 (UK GOVERNMENT SAFETY AGENCY) 4% glucose solution and 0.18% sodium chloride solution should not be used in routine practice Intra- and postoperatively use only isotonic solutions
 Intraoperative Fluid Therapy - ECF Tonicity Na & Cl Bicarbonate, Ca, K – Lactated Ringer – Phys. Solution (Normal saline) Na (154) Large amounts - hyperchloremic metabolic acidosis - no complications (adults)
Intraoperative Fluid Therapy - ECF Tonicity Na & Cl Bicarbonate, Ca, K – Lactated Ringer – Phys. Solution (Normal saline) Na (154) Large amounts - hyperchloremic metabolic acidosis - no complications (adults)
 Intraoperative fluid therapy - glucose Hypoglycemia Stress hormones Autoregulation of cerebral blood flow (300%) Transition to the Krebs cycle with disruption of homeostasis Hyperglycemia Autoregulation of cerebral blood flow Mortality (3 -6) Osmotic diuresis
Intraoperative fluid therapy - glucose Hypoglycemia Stress hormones Autoregulation of cerebral blood flow (300%) Transition to the Krebs cycle with disruption of homeostasis Hyperglycemia Autoregulation of cerebral blood flow Mortality (3 -6) Osmotic diuresis
 Control randomized blind studies of LR with 0.9% or 1% dextrose Without hypoglycemia 1 hour after surgery Glucose level at the end of surgery increased (stress) Norm in the group without dextrose
Control randomized blind studies of LR with 0.9% or 1% dextrose Without hypoglycemia 1 hour after surgery Glucose level at the end of surgery increased (stress) Norm in the group without dextrose
 Intraoperative fluid therapy - Glucose Phys. solution (0.3% and 0.4%) and dextrose (5% and 2.5%) Hongnat J. M., et al. Evaluation of current pediatric guidelines for fluid therapy using two different dextrose hydrating solutions. Paediatr. Anaesth. 1991: 1: 95 -100 Lactated Ringer and dextrose (1% and 2.5%) Dubois M. C. Lactated Ringer with 1% dextrose: an appropriate solution for peri-operative fluid therapy in children. Paediatr. Anaesth. 1992; 2: 99 -104 1. Less concentrated solutions with high content dextrose - greater risk of hyperglycemia and hyponatremia 2. Optimum-Lactated Ringer and dextrose 1%
Intraoperative fluid therapy - Glucose Phys. solution (0.3% and 0.4%) and dextrose (5% and 2.5%) Hongnat J. M., et al. Evaluation of current pediatric guidelines for fluid therapy using two different dextrose hydrating solutions. Paediatr. Anaesth. 1991: 1: 95 -100 Lactated Ringer and dextrose (1% and 2.5%) Dubois M. C. Lactated Ringer with 1% dextrose: an appropriate solution for peri-operative fluid therapy in children. Paediatr. Anaesth. 1992; 2: 99 -104 1. Less concentrated solutions with high content dextrose - greater risk of hyperglycemia and hyponatremia 2. Optimum-Lactated Ringer and dextrose 1%
 Recommendations Crystalloids - solution of choice D 5% 0.45 Na. Cl, D 5% 33 Na. CL…. should not be used routinely in healthy children LR - with low risk of hypoglycemia LR 1% - solution for hypo/hyperglycemia
Recommendations Crystalloids - solution of choice D 5% 0.45 Na. Cl, D 5% 33 Na. CL…. should not be used routinely in healthy children LR - with low risk of hypoglycemia LR 1% - solution for hypo/hyperglycemia
 Polyionique B 66 and B 26 Composition (mmol/l) Lactated Polyionique B 66 Ringer Polyionique B 26 Na 130 120 68 K 4. 0 4. 2 27 Ca 1. 5 2. 8 0 Cl 109 108. 3 95 Lactate 28 20. 7 0 Dextrose 0 50. 5 277 > 3 years Add. I/O losses; HP and younger age P/O Normovolemia
Polyionique B 66 and B 26 Composition (mmol/l) Lactated Polyionique B 66 Ringer Polyionique B 26 Na 130 120 68 K 4. 0 4. 2 27 Ca 1. 5 2. 8 0 Cl 109 108. 3 95 Lactate 28 20. 7 0 Dextrose 0 50. 5 277 > 3 years Add. I/O losses; HP and younger age P/O Normovolemia
 Recommendations (France) Polyionique B 66 - for routine intraoperative fluid therapy in children - Reduces the risk of severe hyponatremia - % glucose - a compromise solution to prevent hypo/hyperglycemia
Recommendations (France) Polyionique B 66 - for routine intraoperative fluid therapy in children - Reduces the risk of severe hyponatremia - % glucose - a compromise solution to prevent hypo/hyperglycemia
 Recommendations Crystalloids are the solution of choice Short operations (myringotomy, ...) – No need Operations 1 -2 hours – 5 -10 ml/kg + blood loss ml/kg Long complex operations – Rule 4 -2 -1 – 10 -20 ml/kg LR/physical solution + blood loss
Recommendations Crystalloids are the solution of choice Short operations (myringotomy, ...) – No need Operations 1 -2 hours – 5 -10 ml/kg + blood loss ml/kg Long complex operations – Rule 4 -2 -1 – 10 -20 ml/kg LR/physical solution + blood loss
 Perioperative fluid therapy Number of hours of fasting x hourly exercise. need – 50% - 1st hour – 25% - 2nd hour – 25% - 3rd hour Furman E., Anesthesiology 1975; 42: 187 -193
Perioperative fluid therapy Number of hours of fasting x hourly exercise. need – 50% - 1st hour – 25% - 2nd hour – 25% - 3rd hour Furman E., Anesthesiology 1975; 42: 187 -193
 Intraoperative fluid therapy - Volume Recommendations according to age and severity of injury 1st hour – 25 ml/kg ≤ 3 years, 15 ml/kg ≥ 4 years Further time (Physical requirement 4 ml/kg/hour + injury) – Light - 6 ml/kg/h – Moderate- 8 ml/kg/h – Severe -10 ml/kg/h + blood loss Berry F., ed. Anesthetic Management of Difficult and Routine Pediatric Patients. , pp. 107 -135. (1986). ,
Intraoperative fluid therapy - Volume Recommendations according to age and severity of injury 1st hour – 25 ml/kg ≤ 3 years, 15 ml/kg ≥ 4 years Further time (Physical requirement 4 ml/kg/hour + injury) – Light - 6 ml/kg/h – Moderate- 8 ml/kg/h – Severe -10 ml/kg/h + blood loss Berry F., ed. Anesthetic Management of Difficult and Routine Pediatric Patients. , pp. 107 -135. (1986). ,
 Intraoperative fluid therapy - Tonicity Isotonic transfer of fluid from the ECF to the non-functional 3rd space >50 ml/kg/h - NEC in premature infants § IVF § ECF 1 ml/kg/h - minor operations fetus NR 4 -6 months 15 -20 ml /kg/chabdominal
Intraoperative fluid therapy - Tonicity Isotonic transfer of fluid from the ECF to the non-functional 3rd space >50 ml/kg/h - NEC in premature infants § IVF § ECF 1 ml/kg/h - minor operations fetus NR 4 -6 months 15 -20 ml /kg/chabdominal
 Recommendations Dependence on surgical trauma Minimum 3 -5 ml/kg/h Moderate 5 -10 ml/kg/h Large 8 -20 ml/kg/h
Recommendations Dependence on surgical trauma Minimum 3 -5 ml/kg/h Moderate 5 -10 ml/kg/h Large 8 -20 ml/kg/h
 Blood loss Calculation of the maximum permissible volume of blood loss MDOC = Weight (kg) x BCC (ml/kg) x (Ht out – 25) Ht medium Ht out – initial hematocrit; Ht avg – average of Ht ref and 25%. Circulating blood volume: Premature newborn 90 – 100 ml/kg; Full-term newborn 80 – 90 ml/kg; Children
Blood loss Calculation of the maximum permissible volume of blood loss MDOC = Weight (kg) x BCC (ml/kg) x (Ht out – 25) Ht medium Ht out – initial hematocrit; Ht avg – average of Ht ref and 25%. Circulating blood volume: Premature newborn 90 – 100 ml/kg; Full-term newborn 80 – 90 ml/kg; Children
 Infusion therapy For small losses, isotonic crystalloids (Ringer, 0.9% Na. Cl, sterofundin) For large losses in the third space, a deficiency of bcc, plasma substitutes (HES, gelofusin) 10 -20 ml/kg are included in the IT composition. If blood loss is > 20% (in newborns > 10%) of the blood volume, blood transfusion is performed. For blood loss > 30% of blood volume, FFP is included in the composition
Infusion therapy For small losses, isotonic crystalloids (Ringer, 0.9% Na. Cl, sterofundin) For large losses in the third space, a deficiency of bcc, plasma substitutes (HES, gelofusin) 10 -20 ml/kg are included in the IT composition. If blood loss is > 20% (in newborns > 10%) of the blood volume, blood transfusion is performed. For blood loss > 30% of blood volume, FFP is included in the composition
 Indications for infusion therapy in children with burns Damage to more than 10% of the body surface area Age up to 2 years
Indications for infusion therapy in children with burns Damage to more than 10% of the body surface area Age up to 2 years
 Emergency measures Fluid Volemic load up to 20 -30 ml/kg/hour Control: diuresis, blood pressure, level of consciousness
Emergency measures Fluid Volemic load up to 20 -30 ml/kg/hour Control: diuresis, blood pressure, level of consciousness
 Parkland formula In the first 24 hours V=4 x body weight x % burn Ringer-Lactate solution, Sterofundin, Ionosteril 50% in the first 8 hours 50% in the next 16 hours
Parkland formula In the first 24 hours V=4 x body weight x % burn Ringer-Lactate solution, Sterofundin, Ionosteril 50% in the first 8 hours 50% in the next 16 hours
 Composition of infusion therapy: Saline solutions (ringer, sterofundin, 0.9% Na. Cl) + plasma expanders. 10% Albumin is prescribed when the albumin fraction in the blood decreases to less than 25 g/l. PSZ: Fibrinogen up to 0.8 g/l; PTI less than 60%; Prolongation of TV or APTT by more than 1.8 times the control
Composition of infusion therapy: Saline solutions (ringer, sterofundin, 0.9% Na. Cl) + plasma expanders. 10% Albumin is prescribed when the albumin fraction in the blood decreases to less than 25 g/l. PSZ: Fibrinogen up to 0.8 g/l; PTI less than 60%; Prolongation of TV or APTT by more than 1.8 times the control
 Colloids vs Crystalloids Isotonic solutions of crystalloids Require a lot, easily pass from the third space to the intravascular Colloids can be prescribed on the second day of therapy, when capillary permeability decreases - will not go into edema Perel P, Roberts I, Pearson M. Colloids versus crystalloids for fluid resuscitation in critically ill patients. Cochrane Database of Systematic Reviews 2007, Issue 4
Colloids vs Crystalloids Isotonic solutions of crystalloids Require a lot, easily pass from the third space to the intravascular Colloids can be prescribed on the second day of therapy, when capillary permeability decreases - will not go into edema Perel P, Roberts I, Pearson M. Colloids versus crystalloids for fluid resuscitation in critically ill patients. Cochrane Database of Systematic Reviews 2007, Issue 4
 Signs of adequate fluid load Decreased tachycardia Warm, pink skin outside the burn surface (SBP 2 -2.5 sec) Diuresis not less than 1 ml/kg/hour Normal indicators R. H, BE +/-2
Signs of adequate fluid load Decreased tachycardia Warm, pink skin outside the burn surface (SBP 2 -2.5 sec) Diuresis not less than 1 ml/kg/hour Normal indicators R. H, BE +/-2
 Hemorrhagic shock Develops as a result of blood loss associated with trauma, surgery, gastrointestinal bleeding, hemolysis; Determining the volume of blood loss is difficult due to the small volume of blood volume; Weakly expressed clinical symptoms shock (pallor, cold sweat, tachycardia, tachypnea) and appear with a loss of blood volume > 20 – 25%; Newborns compensate for hypovolemia worse - a 10% decrease in blood volume leads to a decrease in LV SV, without an increase in heart rate. Hb. F
Hemorrhagic shock Develops as a result of blood loss associated with trauma, surgery, gastrointestinal bleeding, hemolysis; Determining the volume of blood loss is difficult due to the small volume of blood volume; Weakly expressed clinical symptoms shock (pallor, cold sweat, tachycardia, tachypnea) and appear with a loss of blood volume > 20 – 25%; Newborns compensate for hypovolemia worse - a 10% decrease in blood volume leads to a decrease in LV SV, without an increase in heart rate. Hb. F
 Objectives of ITT for blood loss Restoration and maintenance of blood volume; Stabilization of hemodynamics and central venous pressure; Normalization of rheology and blood microcirculation; Restoration of WWTP and VEB; Restoration of coagulation factor deficiency; Restoring the oxygen transport function of the blood.
Objectives of ITT for blood loss Restoration and maintenance of blood volume; Stabilization of hemodynamics and central venous pressure; Normalization of rheology and blood microcirculation; Restoration of WWTP and VEB; Restoration of coagulation factor deficiency; Restoring the oxygen transport function of the blood.
 Tactics intensive care For blood loss of 15–20% of the blood volume, only saline solutions are used; Blood loss of more than 20 - 25% of the volume of blood volume is accompanied by SLN and symptoms of hypovolemic shock and is compensated with saline solutions, plasma substitutes (gelofusin, HES), erythromass; If blood loss exceeds 30–40% of the blood volume, FFP 10–15 ml/kg is included in the IT program. These recommendations are indicative only. In a specific clinical situation, it is necessary to focus on blood pressure, central venous pressure, red blood cell values Hb, Ht, and coagulogram.
Tactics intensive care For blood loss of 15–20% of the blood volume, only saline solutions are used; Blood loss of more than 20 - 25% of the volume of blood volume is accompanied by SLN and symptoms of hypovolemic shock and is compensated with saline solutions, plasma substitutes (gelofusin, HES), erythromass; If blood loss exceeds 30–40% of the blood volume, FFP 10–15 ml/kg is included in the IT program. These recommendations are indicative only. In a specific clinical situation, it is necessary to focus on blood pressure, central venous pressure, red blood cell values Hb, Ht, and coagulogram.
 Principles of blood transfusion therapy in children The main document regulating the use of blood components in children is order No. 363; The basic principles of blood transfusions are not fundamentally different from those in adult patients, except for the neonatal period;
Principles of blood transfusion therapy in children The main document regulating the use of blood components in children is order No. 363; The basic principles of blood transfusions are not fundamentally different from those in adult patients, except for the neonatal period;
 Transfusion of erythrocyte-containing components. The main goal is to restore the oxygen transport function of the blood as a result of a decrease in the number of red blood cells. Indications. Acute anemia due to developed bleeding due to injuries, surgical operations, diseases of the gastrointestinal tract. Blood transfusion is indicated for acute blood loss > 20% of blood volume. Nutritional anemia, occurring in severe form and associated with deficiency of iron, vitamin B 12, folic acid; Anemia, with depression of hematopoiesis (hemoblastosis, aplastic syndrome, acute and chronic leukemia, renal failure, etc.), leading to hypoxemia. Anemia due to hemoglobinopathy (thalassemia, sickle cell anemia). Hemolytic anemia (autoimmune, HUS)
Transfusion of erythrocyte-containing components. The main goal is to restore the oxygen transport function of the blood as a result of a decrease in the number of red blood cells. Indications. Acute anemia due to developed bleeding due to injuries, surgical operations, diseases of the gastrointestinal tract. Blood transfusion is indicated for acute blood loss > 20% of blood volume. Nutritional anemia, occurring in severe form and associated with deficiency of iron, vitamin B 12, folic acid; Anemia, with depression of hematopoiesis (hemoblastosis, aplastic syndrome, acute and chronic leukemia, renal failure, etc.), leading to hypoxemia. Anemia due to hemoglobinopathy (thalassemia, sickle cell anemia). Hemolytic anemia (autoimmune, HUS)
 Transfusion of erythrocyte-containing components. In the presence of anemia not associated with o. blood loss, the solution to the issue is based on the following factors: 1. The presence of signs of hypoxemia (shortness of breath, tachycardia) and tissue hypoxia (lactate, metabolic acidosis); 2. The child has cardiopulmonary pathology; 3. Methods are not effective conservative therapy. Indications in the presence of tissue hypoxia Hb
Transfusion of erythrocyte-containing components. In the presence of anemia not associated with o. blood loss, the solution to the issue is based on the following factors: 1. The presence of signs of hypoxemia (shortness of breath, tachycardia) and tissue hypoxia (lactate, metabolic acidosis); 2. The child has cardiopulmonary pathology; 3. Methods are not effective conservative therapy. Indications in the presence of tissue hypoxia Hb
 Normal Hb values At birth 140 - 240 g/l 3 months 80 -140 g/l 6 months-6 years 100 -140 g/l 7 -12 years 110 -160 g/l Adults 115 -180 g/l Anaesth Intensive Care Med. 2012; 13:20 -27
Normal Hb values At birth 140 - 240 g/l 3 months 80 -140 g/l 6 months-6 years 100 -140 g/l 7 -12 years 110 -160 g/l Adults 115 -180 g/l Anaesth Intensive Care Med. 2012; 13:20 -27
 Indications for blood transfusion Up to 4 months less than 120 g/l for premature or full-term infants with anemia; 110 g/l for children with chronic oxygen dependence; 120 -140 g/l for severe lung pathology; 70 g/l for late anemia in stable children; 120 g/l for acute blood loss of more than 10% of the blood volume. Anaesth Intensive Care Med. 2012; 13:20 -27
Indications for blood transfusion Up to 4 months less than 120 g/l for premature or full-term infants with anemia; 110 g/l for children with chronic oxygen dependence; 120 -140 g/l for severe lung pathology; 70 g/l for late anemia in stable children; 120 g/l for acute blood loss of more than 10% of the blood volume. Anaesth Intensive Care Med. 2012; 13:20 -27
 Indications for blood transfusion Over 4 months 70 g/l for stable children; 70 -80 g/l for critically ill children; 80 g/l for perioperative bleeding; 90 g/l for blue heart defects; Thalassemia (with lack of activity bone marrow) 90 g/l. Hemolytic anemia 70 -90 g/l or more than 90 g/l during a crisis. For surgical interventions 90 -110 g/l. The amount of pathological Hb is no more than 30% and less than 20% in thoracic neurosurgery Anaesth Intensive Care Med. 2012; 13:20 -27
Indications for blood transfusion Over 4 months 70 g/l for stable children; 70 -80 g/l for critically ill children; 80 g/l for perioperative bleeding; 90 g/l for blue heart defects; Thalassemia (with lack of activity bone marrow) 90 g/l. Hemolytic anemia 70 -90 g/l or more than 90 g/l during a crisis. For surgical interventions 90 -110 g/l. The amount of pathological Hb is no more than 30% and less than 20% in thoracic neurosurgery Anaesth Intensive Care Med. 2012; 13:20 -27
 Reduce blood transfusions Maximize hemoglobin Acute normovolemic hemodilution Prevention of high venous pressure Use of tourniquets where possible Surgical technique (diathermy, adhesives) Hypervolemic hemodilution Tranexamic acid Use of Cellsavers Anaesth Intensive Care Med. 2012; 13:20 -27
Reduce blood transfusions Maximize hemoglobin Acute normovolemic hemodilution Prevention of high venous pressure Use of tourniquets where possible Surgical technique (diathermy, adhesives) Hypervolemic hemodilution Tranexamic acid Use of Cellsavers Anaesth Intensive Care Med. 2012; 13:20 -27
 Indications for PSZ transfusion: DIC syndrome; acute massive blood loss of more than 30% of the circulating blood volume with the development hemorrhagic shock; liver diseases accompanied by a decrease in the production of plasma coagulation factors, if there is bleeding, or before surgery; burn disease accompanied by plasma loss and DIC syndrome; exchange plasmapheresis. Coagulogram: - when fibrinogen decreases to 0.8 g/l; - when the PTI decreases to less than 60%; - when the TV or APTT is prolonged by more than 1.8 times the control.
Indications for PSZ transfusion: DIC syndrome; acute massive blood loss of more than 30% of the circulating blood volume with the development hemorrhagic shock; liver diseases accompanied by a decrease in the production of plasma coagulation factors, if there is bleeding, or before surgery; burn disease accompanied by plasma loss and DIC syndrome; exchange plasmapheresis. Coagulogram: - when fibrinogen decreases to 0.8 g/l; - when the PTI decreases to less than 60%; - when the TV or APTT is prolonged by more than 1.8 times the control.
 Features of PSZ transfusion. PSZ dose 10 – 15 ml/kg; For DIC with hemorrhagic syndrome, 20 ml/kg; About liver diseases with a decrease in the level of coagulation factors and bleeding 15 ml/kg, followed by repeated transfusion h/w 4 - 8 hours 5 - 10 ml/kg; Preparation of PSZ in a defrost T 37 o. C After defrosting d.b. used within an hour.
Features of PSZ transfusion. PSZ dose 10 – 15 ml/kg; For DIC with hemorrhagic syndrome, 20 ml/kg; About liver diseases with a decrease in the level of coagulation factors and bleeding 15 ml/kg, followed by repeated transfusion h/w 4 - 8 hours 5 - 10 ml/kg; Preparation of PSZ in a defrost T 37 o. C After defrosting d.b. used within an hour.
 Transfusion of platelet concentrate. Platelets less than 5 x 109 l with or without bleeding and bleeding; Platelets less than 20 x 109 l if the patient has a septic condition, disseminated intravascular coagulation; Platelets less than 50 x 109 l with severe hemorrhagic syndrome, the need for surgical interventions or other invasive diagnostic procedures. Platelets less than 10 x 109 l in patients with acute leukemia during chemotherapy. Prophylactic transfusion of platelet concentrate with deep thrombocytopenia (20 -30 x 109/l) of amegakaryocytic nature without signs of spontaneous bleeding is indicated in the presence of sepsis against the background of agranulocytosis and disseminated intravascular coagulation.
Transfusion of platelet concentrate. Platelets less than 5 x 109 l with or without bleeding and bleeding; Platelets less than 20 x 109 l if the patient has a septic condition, disseminated intravascular coagulation; Platelets less than 50 x 109 l with severe hemorrhagic syndrome, the need for surgical interventions or other invasive diagnostic procedures. Platelets less than 10 x 109 l in patients with acute leukemia during chemotherapy. Prophylactic transfusion of platelet concentrate with deep thrombocytopenia (20 -30 x 109/l) of amegakaryocytic nature without signs of spontaneous bleeding is indicated in the presence of sepsis against the background of agranulocytosis and disseminated intravascular coagulation.
 Transfusion of platelet concentrate with increased destruction of platelets of immune origin is not indicated. In case of thrombocytopathies, transfusion of platelet concentrate is indicated only in urgent situations - in case of massive bleeding, operations.
Transfusion of platelet concentrate with increased destruction of platelets of immune origin is not indicated. In case of thrombocytopathies, transfusion of platelet concentrate is indicated only in urgent situations - in case of massive bleeding, operations.
 Blood transfusion therapy in newborns. In the neonatal period, anemia is predisposed by: 1. Anatomical and physiological features: Change of Hb synthesis from fetal to adult; Short cycle life of an erythrocyte (12 – 70 days); Low erythropoietin levels; Red blood cells have reduced filterability (increased destruction). 2. Prematurity (lower red blood counts and more severe anemia); 3. Iatrogenic anemia due to repeated blood sampling for research.
Blood transfusion therapy in newborns. In the neonatal period, anemia is predisposed by: 1. Anatomical and physiological features: Change of Hb synthesis from fetal to adult; Short cycle life of an erythrocyte (12 – 70 days); Low erythropoietin levels; Red blood cells have reduced filterability (increased destruction). 2. Prematurity (lower red blood counts and more severe anemia); 3. Iatrogenic anemia due to repeated blood sampling for research.
 Indications. at birth Ht 10% of bcc (↓ SV without heart rate); in the presence of clinically pronounced signs of severe anemia - hypoxemia (tachycardia > 180 and/or tachypnea > 80) and higher Ht values.
Indications. at birth Ht 10% of bcc (↓ SV without heart rate); in the presence of clinically pronounced signs of severe anemia - hypoxemia (tachycardia > 180 and/or tachypnea > 80) and higher Ht values.
 Rules for blood transfusions in newborns: All transfusions in newborns are considered massive. Only filtered or washed red blood cells are transfused according to individual selection. The rate of red blood cell transfusion is 2-5 ml/kg body weight per hour under mandatory monitoring of hemodynamics and respiration. For rapid transfusions (0.5 ml/kg body weight per minute), it is necessary to pre-warm the erythromass. ABO testing is carried out only with the recipient's red blood cells, using anti-A and anti-B reagents, since natural antibodies in early age usually not detected. For HDN caused by anti-D antibodies, only Rh is transfused - negative blood. If the pathogenic antibodies are not anti-D antibodies, the newborn can be transfused with Rh-positive blood.
Rules for blood transfusions in newborns: All transfusions in newborns are considered massive. Only filtered or washed red blood cells are transfused according to individual selection. The rate of red blood cell transfusion is 2-5 ml/kg body weight per hour under mandatory monitoring of hemodynamics and respiration. For rapid transfusions (0.5 ml/kg body weight per minute), it is necessary to pre-warm the erythromass. ABO testing is carried out only with the recipient's red blood cells, using anti-A and anti-B reagents, since natural antibodies in early age usually not detected. For HDN caused by anti-D antibodies, only Rh is transfused - negative blood. If the pathogenic antibodies are not anti-D antibodies, the newborn can be transfused with Rh-positive blood.


 See Also – Pediatric Dehydration Replace Phase 1 Acute Resuscitation – Give LR OR NS at 10 -20 ml/kg IV over 30 -60 minutes – May repeat bolus until circulation stable Calculate 24 hour maintenance requirements – Formula First 10 kg: 4 cc/kg /hour (100 cc/kg/24 hours) Second 10 kg: 2 cc/kg/hour (50 cc/kg/24 hours) Remainder: 1 cc/kg/hour (20 cc/kg/24 hours) – Example: 35 Kilogram Child Hourly: 40 cc/h + 20 cc/h + 15 cc/h = 75 cc/hour Daily: 1000 cc + 500 cc + 300 cc = 1800 cc/day Calculate Deficit (See Pediatric Dehydration) – Mild Dehydration: 4% deficit (40 ml/kg) – Moderate Dehydration: 8% deficit (80 ml/kg) – Severe Dehydration: 12% deficit (120 ml/kg) Calculate remaining deficit – Subtract fluid resucitation given in Phase 1 Calculate Replacement over 24 hours – First 8 hours: 50% Deficit + Maintenance – Next 16 hours: 50% Deficit + Maintenance Determine Serum Sodium Concentration – Pediatric Hypertonic Dehydration (Serum Sodium > 150) – Pediatric Isotonic Dehydration – Pediatric Hypotonic Dehydration (Serum Sodium
See Also – Pediatric Dehydration Replace Phase 1 Acute Resuscitation – Give LR OR NS at 10 -20 ml/kg IV over 30 -60 minutes – May repeat bolus until circulation stable Calculate 24 hour maintenance requirements – Formula First 10 kg: 4 cc/kg /hour (100 cc/kg/24 hours) Second 10 kg: 2 cc/kg/hour (50 cc/kg/24 hours) Remainder: 1 cc/kg/hour (20 cc/kg/24 hours) – Example: 35 Kilogram Child Hourly: 40 cc/h + 20 cc/h + 15 cc/h = 75 cc/hour Daily: 1000 cc + 500 cc + 300 cc = 1800 cc/day Calculate Deficit (See Pediatric Dehydration) – Mild Dehydration: 4% deficit (40 ml/kg) – Moderate Dehydration: 8% deficit (80 ml/kg) – Severe Dehydration: 12% deficit (120 ml/kg) Calculate remaining deficit – Subtract fluid resucitation given in Phase 1 Calculate Replacement over 24 hours – First 8 hours: 50% Deficit + Maintenance – Next 16 hours: 50% Deficit + Maintenance Determine Serum Sodium Concentration – Pediatric Hypertonic Dehydration (Serum Sodium > 150) – Pediatric Isotonic Dehydration – Pediatric Hypotonic Dehydration (Serum Sodium
| CHILDREN'S AGE | WEIGHT IN KG | TOTAL FLUID REQUIREMENT | |
| PER DAY (ML) | PER 1 KG OF WEIGHT | ||
| 3 days | 3,0 | 250 — 300 | 80 – 100 |
| 10 days | 3,2 | 400 — 500 | 125 – 150 |
| 3 months | 5,4 | 750 — 850 | 140 – 160 |
| 6 months | 7,3 | 950 — 1100 | 130 – 155 |
| 9 months | 8,6 | 1100 — 1250 | 125 – 145 |
| 1 year | 9,5 | 1300 — 1500 | 120 – 135 |
| 2 years | 11,8 | 1350 — 1500 | 115 – 125 |
| 4 years | 16,2 | 1600 — 1800 | 100 – 110 |
| 6 years | 20,0 | 1800 — 2000 | 90 – 100 |
| 10 years | 28,7 | 2000 — 2500 | 70 – 80 |
| 14 years | 45,0 | 2200 — 2700 | 40 — 50 |
The constancy of water-electrolyte metabolism is maintained by osmotic and oncotic pressure. Osmotic pressure in the extracellular space is provided mainly by sodium and chlorine, in the intracellular space by potassium, oncotic pressure created in the vascular bed and in the cell is supported by proteins.
The main electrolytes of the cell are potassium, calcium, magnesium; the extracellular space predominantly contains sodium and chlorine.
Sodium (normal – 135 – 155 mmol/l in plasma) is the main ion on which the osmotic pressure of the internal environment depends.
Potassium (norm – 3.5 – 6.5 mmol/l in plasma) is indispensable in performing intracellular functions. It is involved in protein and carbohydrate metabolism and in neuromuscular conduction. IN cell membrane There is a potassium-sodium pump that pushes sodium ions out of the cell in exchange for potassium ions carried into the cell. The rhythm of operation of this pump strictly depends on the energy potential of the cell.
BCC in an adult is 70 ml/kg or 5–8% of body weight; in infants this figure varies from 75 to 110 ml/kg, averaging 10–12% of body weight.
Ensuring the balance of water-electrolyte metabolism is a complex neurohumoral mechanism, which involves:
State osmotic pressure controlled osmo receptors,- and oncotic - by volume receptors, which transmit information to the central nervous system about the state of osmotic pressure and tissue hydration, fluctuations in bcc.
Osmo- and volumetric receptors are located in the vessels, interstitial space, in the form of islands in the right atrium and the cranium.
In the area of the hypothalamus there is a center of thirst and antidiuresis, the latter is associated with the posterior lobe of the pituitary gland, where it produces antidiuretic hormone(ADH) – vasopressin. ADH controls isotonia by conserving water volume; aldosterone - by regulating salt concentration.
Already with a loss of 1.5 - 2% of water, osmotic hypertension develops as a result of which:
This is the body’s stereotypical reaction to any increase in the osmotic pressure of the extracellular fluid. As a result, salts are diluted and isotonicity is restored.
On the other hand, a decrease in BCC during hypovolemia is perceived by receptors that, through the system renin-angiotensin leads to vasoconstructions and stimulation of secretion aldosterone– hormone of the adrenal cortex. Vasospasm causes a decrease in fluid filtration. Aldosterone promotes reabsorption sodium in the renal tubules and potassium excretion. As a result, blood osmolarity increases, water is retained in the body, and hypovolemia decreases. Internal environment returns to isotonia. Excess water causes inhibition of aldosterone secretion. This results in decreased sodium reabsorption and increased excretion of sodium and water. In turn, a decrease in sodium concentration in the blood inhibits the secretion of ADH - excess water is released.
The lability of water-electrolyte metabolism, the predominance of extracellular fluid and its rapid loss, high permeability of renal vessels in infants for a number of other reasons explains the ease of dehydration.
The need for water in a healthy or sick body is determined by the total amount of water excreted from the body through urine, through the skin, from the surface of the lungs, and with feces. For adults, the need for water is 40 ml/kg per day (V. A. Negovsky, A. M. Gurvich, E. S. Zolotokrylina, 1987), the daily need for sodium is 1.5 mmol/kg, for calcium - approximately 9 mmol (10 ml of 10% solution of gluconate or calcium chloride), and the daily requirement for magnesium is 0.33 mmol/kg. The amount of 25% magnesium sulfate can be determined by the formula:
Total daily requirement (MgSO4) in mmol: 2 = ml/day.
It is advisable to administer potassium chloride in a solution of glucose with insulin, but its concentration should not exceed 0.75% and the rate of administration 0.5 mmol/(kg hour). The total potassium load should not exceed 2-3 mmol/(kg day).
The physiological need for fluid is compensated with saline solutions and 5-10% glucose solution in a ratio of 1:2 or 1:1.
The next stage of implementation infusion program is to compensate for the deficiency of fluid and ions and current pathological losses in the patient’s body. It should be noted that this problem must be solved first, since this is where the success of treatment lies largely.
There are physiological and pathological losses. Thus, perspiration in adults is 0.5 ml/kg per hour. Loss through diuresis is normally 1 ml/kg per hour.
Knowledge of physiological losses is especially important and necessary when conducting infusion therapy in patients with renal failure, since the given figures for daily fluid requirements already include physiological losses. It is equally important to take into account pathological losses, which can reach significant values. Thus, with hyperthermia (more than 37°) and an increase in body temperature by 1°, water loss increases by an average of 500 ml per day. Water excreted through sweat contains 20-25 mOsmol/L Na+ and 15-35 mOsmol/L SG. Losses may increase with fever, thyrotoxic crises, treatment with certain medicines(pilocarpine), high ambient temperatures.
Water loss in feces in an adult is normally about 200 ml/day. Digestion is accompanied by the release of about 8-10 liters of water with ions dissolved in it into the lumen of the stomach and intestines. In a healthy intestine, almost all of this volume is reabsorbed.
In pathological conditions (diarrhea, vomiting, fistulas, intestinal obstruction), the body loses significant amount water and ions. When absorption processes from the intestine are disrupted, transcellular pools are formed, sequestering a large number of water and electrolytes. For an approximate correction, it is recommended to increase the volume of fluid by 20 ml/(kg day) with the development of stage II intestinal paresis. III degree- by 40 ml/(kg day). Corrective solutions must contain sodium, potassium, chlorine, etc. ions.
Frequent vomiting causes a water deficiency of an average of 20 ml/(kg day), and correction is best done with solutions containing chlorides and potassium.
For moderate diarrhea, fluid replacement is recommended at the rate of 30-40 ml/(kg day), for severe diarrhea - 60-70 ml/(kg day), and for profuse diarrhea - up to 120-40 ml/(kg day) with solutions containing ions sodium, potassium, chlorine, magnesium.
In case of hyperventilation, it is advisable to administer 15 ml/(kg day) of glucose solution for every 20 respiratory movements above normal. When performing mechanical ventilation without adequate humidification, up to 50 ml/hour is lost, i.e. ventilation with a RO-6 type device during the day requires additional administration of 1.5 to 2 liters of fluid.
The most ideal and most competent way to correct pathological losses is to determine the composition of the lost media and their quantity. In this case, even using official solutions, existing violations can be corrected quite accurately.
When calculating and selecting various infusion media, some difficulties arise when converting the amount of a substance contained in a solution into mmol and vice versa. Therefore, below we present such ratios for the most commonly used substances.
So, 1 ml contains:
7.4% KCl solution - 1 mmol K+ and 1 mmol Cl‾
3.7% KCl solution - 0.5 mmol K+ and 0.5 mmol Cl‾
5.8% NaCl solution - 1 mmol Na+ and 1 mmol Cl‾
8.4% NaHCO3 solution - 1 mmol Na+ and 1 mmol HCO3‾
4.2% NaHCO3 solution - 0.5 mmol Na+ and 0.5 mmol HCO‾
10% CaCl2 solution - 0.9 mmol Ca++ and 1.8 mmol Cl‾
10% NaCl solution -1.7 mmol Na+ and 1.7 mmol Cl‾
25% MgSO4 solution - 2.1 mmol Mg++ and 2.1 mmol SO4 ²‾
1 mole is equal to:
For successful therapy It is important to determine the ratio of glucose to saline solutions. This ratio will depend on the predominance of water or electrolyte loss. With isotonic dehydration, it is advisable to maintain the ratio of salt-free solutions to salt solutions at 1:1, with water deficiency - 4:1, salt deficiency - 1:2.
The volume of colloids depends, firstly, on the severity of hemodynamic disorders and the state of volemia; secondly, from the need to administer blood substitutes for vital reasons (for example, in the presence of bleeding - administration of plasma, blood).
The choice of the so-called “starting solution” will also depend on the degree of dehydration and its form. Let's clarify this idea. The third degree of dehydration occurs with severe hemodynamic disturbances and should be considered as hypovolemic shock. In this regard, despite the form of dehydration, treatment measures should begin with drugs that create a volemic effect (albumin, rheopolyglucin, hemodez), after which it is necessary to proceed to the administration of fluids, depending on the form of dehydration.
Thus, it is advisable to begin the treatment of extracellular dehydration (salt deficiency exicosis) with the introduction isotonic solution sodium chloride. Administration of 5% glucose is contraindicated, since its rapid movement into the intracellular sector can cause brain edema. On the contrary, for cellular dehydration, a 5% glucose solution is recommended as a starting solution. Causing some hypotonicity of the extracellular sector, it ensures the saturation of the intracellular space with water. In case of total (general) dehydration syndrome, it is recommended to begin therapy with an isotonic glucose solution, followed by a transition to the administration of isotonic saline solutions.
When performing infusion therapy during surgery caesarean section or during childbirth, it must be remembered that the administration of glucose solutions before the birth of the child is indicated only for women with initially low sugar levels. This is dictated by the fact that the supply of glucose to the fetus through the uteroplacental bloodstream causes hyperinsulinemia, which, after the fetus is removed and the supply of glucose from the mother is stopped, can cause hypoglycemia and deterioration of the condition of the newborn. After the baby is removed, glucose and saline are usually administered in a 1:1 ratio.
The total volume of fluid required to correct the deficiency and daily requirement depends on the degree of dehydration. An important criterion for its determination are clinical and laboratory data.
The next task that needs to be solved is determining the time during which it is planned to correct dehydration. It is advisable to adhere to the principle that the total volume of fluid administered (enterally and intravenously) should be within 5-9% of body weight and weight gain should not exceed these figures, because they indicate the limit of the compensatory capabilities of the cardiovascular and urinary systems.
According to V.M. Sidelnikov (1983), the deficit of water and salts should be compensated for in 24-36 hours, and 60% of the water deficit should be introduced within the first 12 hours. In patients with heart failure, this period can be increased to 3 - 5 days. Finberg (1980) recommends administering half of the daily requirement in 6-8 hours, and the rest, plus the volume of pathological losses, in the remaining hours before the end of the day.
Lysenkov S.P., Myasnikova V.V., Ponomarev V.V.
Emergency conditions and anesthesia in obstetrics. Clinical pathophysiology and pharmacotherapy

The meaning of life is related to the question “What to live for”, and not to the question of how to maintain life. A person's attitude is...

A mushroom is a living organism that forms a separate kingdom of the same name. For a long time they were classified as part of the plant kingdom. But in...

For lovers of “quiet” hunting, mushroom season begins in early summer and lasts until late autumn. And rarely do they...
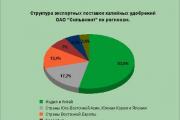
Aleshnikova, V.I. Use of professional consultants. - M.: Infra-M, 1999. - 240 p. 2. Beich, E....

Orange juice. The symbolic meaning of orange juice in dream books is pleasure and temptation. Quite often we...

We most often overcome all kinds of difficulties encountered along the path of life. Of course, for this we make...

This year your patron Neptune will be in your constellation and this is a good sign, because you will...

1993 who? 1993 is the year of which animal? — According to the Chinese horoscope, 1873, 1933, 1993 belonged to the years of the Black...

Wave-particle duality of light means that light simultaneously has the properties of continuous...

The role of biology is enormous in our world. Although it is not one of the priority subjects, most schoolchildren and...

Amines are organic derivatives of ammonia containing an NH 2 amino group and an organic radical. In general...

How to answer questions in Part BThe second part of the social studies work consists of 7 tasks with a short answer....

Form TORG-15 is drawn up in the case when during transportation, movement between and within the warehouse, when...

Nutritionists say that for good health and a slim figure, you must include snacks in your...

A mushroom is a living organism that forms a separate kingdom of the same name. For a long time they were classified as a kingdom...

For lovers of “quiet” hunting, mushroom season begins in early summer and lasts until late autumn. And rarely do they...