Dream interpretation of a dead man being alive
Dream interpretation is an ancient art that allows you to at least assess the psychological status of a person, because...
Today, three in one hundred adults and two in five hundred children are diagnosed with obsessive-compulsive disorder. This is a disease that requires mandatory treatment. We suggest that you familiarize yourself with the symptoms of ACS, the causes of its occurrence, as well as possible options treatment.
Obsessive-compulsive syndrome (or disorder) is constantly repeating identical obsessive involuntary thoughts and (or) actions (rituals). This condition is also called obsessive-compulsive disorder.
The name of the disorder comes from two Latin words:
Doctors and scientists began to be interested in the syndrome back in the 17th century:
According to modern research, obsessive syndrome characterized as a neurosis, that is, it is not a disease in the literal sense of the word.
Obsessive-compulsive syndrome can be schematically depicted as the following sequence of situations: obsessions (obsessive thoughts) - psychological discomfort (anxiety, fears) - compulsions (obsessive actions) - temporary relief, after which everything repeats again.
Depending on the accompanying symptoms, obsessive syndrome can be of several types:
Depending on the time of manifestation, ACS can be:
Experts do not give a clear answer as to why obsessive syndrome may appear. In this regard, there is only an assumption that some biological and psychological factors influence the development of ACS.
Biological reasons:

Psychological reasons:
There is a high risk of developing obsessive syndrome in people whose family has already had similar cases - hereditary predisposition. That is, if there is a person in the family diagnosed with ACS, then the probability that his immediate offspring will have the same neurosis is from three to seven percent.
Also susceptible to ACS next type personalities:
According to statistics, there is no division in the number of patients with obsessive-compulsive disorder syndrome between men and women. But there is a tendency that neurosis most often begins to manifest itself in people aged 15 to 25 years.
The main symptoms of obsessive-compulsive disorder include the appearance of anxious thoughts and monotonous daily activities (for example, constant fear about an incorrectly spoken word or fear of germs, which forces you to wash your hands frequently). Accompanying symptoms may also appear:


How to diagnose obsessive-compulsive disorder? Symptoms of the disease can manifest differently in each person.
The most common obsessions are:
Common obsessive behaviors include:
Children are susceptible to obsessive-compulsive disorder much less frequently than adults. But the symptoms are similar, only adjusted for age:

Diagnosis of obsessive-compulsive syndrome consists of identifying those very obsessive thoughts and actions that have occurred throughout long period time (at least half a month) and are accompanied by a depressed state or depression.
Among the characteristics of obsessive symptoms for diagnosis, the following should be highlighted:
The difficulty is that it is often difficult to separate obsessive-depressive syndrome from simple ACS, since their symptoms occur almost simultaneously. When it is difficult to determine which of them appeared earlier, then depression is considered to be the primary disorder.
The test will help you identify the diagnosis of obsessive-compulsive syndrome. As a rule, it contains a number of questions related to the type and duration of actions and thoughts characteristic of a patient with ACS. For example:
For a more accurate diagnosis and determination of the severity of the disorder, this list of questions can be much longer.
The results depend on the number of points scored. Most often, the more of them, the higher the likelihood of having obsessive-compulsive syndrome.
For help in treating ACS, you should contact a psychiatrist, who will not only help in making an accurate diagnosis, but will also be able to identify the dominant type of obsessive disorder.
How can you generally defeat obsessive syndrome? Treatment of ACS involves a series of psychological therapeutic measures. Medicines fade into the background here, and often they can only maintain the result achieved by the doctor.

As a rule, tricyclic and tetracyclic antidepressants are used (for example, Melipramin, Mianserin and others), as well as anticonvulsants.
If there are metabolic disorders that are necessary for the normal functioning of brain neurons, then the doctor prescribes special drugs for example, Fluvoxamine, Paroxetine, and so on.
Hypnosis and psychoanalysis are not used as therapy. In the treatment of obsessive-compulsive disorder, cognitive-behavioral approaches are used, which are more effective.
The goal of this therapy is to help the patient stop focusing on obsessive thoughts and ideas, gradually drowning them out. The principle of operation is as follows: the patient should focus not on anxiety, but on refusing to perform the ritual. Thus, the patient no longer experiences discomfort from obsession, but from the result of inaction. The brain switches from one problem to another, and after several such approaches, the urge to perform obsessive actions subsides.
Among other well-known methods of therapy, in addition to cognitive behavioral, the “thought stopping” technique is also used in practice. The patient, at the moment of an obsession or action, is advised to mentally say to himself “Stop!” and analyze everything from the outside, trying to answer the following questions:
The list of questions goes on. The main thing is that their goal is to analyze the situation from all sides.
There is also the possibility that the psychologist will decide to use another treatment method as an alternative or as additional help. This depends on the specific case and its severity. For example, this could be family or group psychotherapy.
Even if you have the best therapist in the world, you still need to make an effort yourself. Quite a few doctors - one of them, Jeffrey Schwartz, a very well-known ACS researcher - note that independent work on your condition is very important.
For this you need:

And most importantly, learn to relax. Learn at least the basics of relaxation. Use meditation, yoga or other methods. They will help reduce the impact of OCD symptoms and the frequency of their occurrence.
Obsessive compulsive disorder is an illness whose causes are rarely on the surface. This syndrome is characterized by the presence of intrusive, persistent thoughts (obsessions), to which the person responds with corresponding actions (compulsions).
Obsessive compulsive is deciphered as follows. Obsession (translated from Latin obsessio - “siege”) - desire or thought, which pops up in my brain all the time. This thought is difficult to control or get rid of, which causes extreme stress.
In obsessive compulsive disorder, the most common intrusive thoughts (obsessions) are:

Almost everyone has experienced such intrusive thoughts. But for people with obsessive compulsive disorder, the level of anxiety from these thoughts is off the charts. And in order to relieve anxiety, a person is often forced perform “protective” actions- compulsions (translated from Latin compello - “to force”).
Compulsions with this disease are a bit like rituals. These are actions that people, in response to an obsession, repeat over and over again to reduce the possibility of harm. Compulsions can be physical (for example, constantly checking whether the door is closed) or mental (for example, saying a phrase in your head).
With OCD, compulsions of mental rituals (special prayers or words that are repeated in a certain order), constant checks (for example, gas valves), and counting are common.
The most common is considered fear of virus infection combined with obsessive cleaning and washing. Out of fear of infection, a person can go to great lengths: he avoids shaking hands, does not touch toilet seats, or door handles. Typically, with obsessive compulsive syndrome, the patient stops washing his hands not when they are already clean, but when, in the end, he feels “relief.”
Avoidance behavior is a core part of obsessive compulsive disorder, which includes:
Obsessive compulsive neurosis is usually accompanied by depression, guilt and shame. In human relationships, illness creates chaos and can affect performance. According to WHO, obsessive compulsive disorder is among the top ten diseases that lead to loss of ability to work. A person with obsessive-compulsive disorder syndrome does not seek help from doctors because he is afraid, embarrassed, or does not know that his illness can be treated, including in a non-drug manner.
Despite numerous studies devoted to obsessive compulsive syndrome, it is still impossible to say for sure what is the main cause of OCD. Behind this state Both psychological and physiological reasons may be responsible.
 Research has shown that obsessive compulsive disorder can be passed down through generations. The study of the problem showed that this disease is moderately hereditary, but no gene has been identified as causing this condition. But a lot of attention deserve SLC1A1 and hSERT genes, they might play a role in OCD syndrome:
Research has shown that obsessive compulsive disorder can be passed down through generations. The study of the problem showed that this disease is moderately hereditary, but no gene has been identified as causing this condition. But a lot of attention deserve SLC1A1 and hSERT genes, they might play a role in OCD syndrome:
Brain imaging techniques have enabled scientists to study activity individual parts brain. It has been revealed that the activity of certain areas of the brain in OCD syndrome has specific activity. The obsessive compulsive disorder syndromes involved are:
Brain scan findings in people with obsessive compulsive disorder. The circuit, which includes the areas described above, regulates behavioral factors such as bodily secretions, sexuality and aggression. The chain activates appropriate behavior, for example, after contact with something unpleasant, washing your hands thoroughly. Normally, after the action, the desire decreases, that is, the person finishes washing his hands and begins to perform another activity.
But in people with obsessive compulsive disorder the brain experiences certain complications with the circuit turned off, it creates communication problems. Compulsions and obsessions continue, leading to repetition of an action.
 Obsessive compulsive disorder can result from autoimmune diseases. Certain cases of rapid development of OCD in children may be due to streptococcal bacteria, which cause dysfunction and inflammation of the basal ganglia.
Obsessive compulsive disorder can result from autoimmune diseases. Certain cases of rapid development of OCD in children may be due to streptococcal bacteria, which cause dysfunction and inflammation of the basal ganglia.
Another study suggested that episodic OCD occurs not due to streptococcal bacteria, but more due to the prevention of antibiotics prescribed to treat the disease.
Taking into account the basic law of behavioral psychology, repetition of a certain behavioral action makes it easier to reproduce in the future.
Patients with obsessive compulsive disorder do nothing but try to avoid things that can activate fear, perform “rituals” or “fight” thoughts to reduce feelings of anxiety. These actions temporarily reduce fear, but in a paradoxical way, according to the law described above, they increase the likelihood of obsessive behavior in the future. It turns out that The main cause of OCD is avoidance.. Instead of coping with fear, it is avoided, which can lead to disastrous consequences.
People who are most susceptible to developing OCD are those who are under stress: they suffer from overwork, end relationships, start new job. For example, a person who calmly used the public toilet at work all the time, in a stressful state, unexpectedly begins to “wind up”, saying that the toilet seat is dirty and you can catch an illness. Then, by association, fear begins to spread to other similar objects: public showers, sinks, etc.
When a person begins to avoid public toilets or perform various cleansing rituals (cleaning door handles, seats, followed by thorough hand washing) instead of enduring fear, then this may develop into a phobia.
 Psychological trauma and stress activate OCD syndrome in people who tend to develop this condition. Studies have shown that obsessive-compulsive neurosis in 55-75% of cases appeared due to the adverse effects of the environment.
Psychological trauma and stress activate OCD syndrome in people who tend to develop this condition. Studies have shown that obsessive-compulsive neurosis in 55-75% of cases appeared due to the adverse effects of the environment.
Statistics prove the fact that many people with symptoms of obsessive-compulsive disorder have experienced traumatic or stressful event. These events can also worsen an existing disorder. Here is a list of the most traumatic environmental causes:
Cognitive theory explains the appearance of OCD syndrome by the inability to correctly interpret thoughts. Many people have intrusive or unwanted thoughts several times a day, but all people who suffer from the disorder significantly exaggerate the importance of such thoughts.
Obsessions in young mothers. For example, a woman who is raising a baby, due to fatigue, may from time to time be visited by thoughts of harming her child. Many, naturally, brush aside these obsessions and do not notice them. People who suffer from the disorder exaggerate the importance of thoughts and take them as a threat: “What if I’m actually capable of this?!”
The woman thinks that she may be a threat to the baby, and this causes anxiety and other negative emotions in her, such as feelings of shame, guilt or disgust.
Fear of one's thoughts sometimes leads to attempts to neutralize the negative emotions that arise from obsessions, for example, by avoiding situations that trigger those thoughts, or by engaging in "rituals" of prayer or excessive purification.
Scientists suggest that people with the disorder give exaggerated meaning to thoughts due to false prejudices that were received in childhood. Among them:

For effective treatment disorders, knowledge of the causes that caused the disease is not so important. It is much more important to know the mechanisms that support OCD. This is the key to overcoming the disorder.
OCD is supported by the following circle: anxiety, obsession and the response to this anxiety.
Constantly, when a person avoids an action or situation, his behavior is “fixed” in the brain in the form of a corresponding neural circuit. The next time in the same situation, he will begin to act in the same way, and accordingly, he will again miss the chance to reduce the activity of neurosis.
Compulsions also become entrenched. A person feels less anxious when he has checked whether the iron is turned off. Accordingly, he will begin to act in the same way in the future.
Impulsive actions and avoidances initially “work”: the person believes that he has prevented harm, and this stops the feeling of anxiety. But in the long term, this creates even more fear and anxiety, as it feeds the obsession.
The OCD patient greatly exaggerates his ability to influence the world and his capabilities. He confident in his power prevent or cause negative events through thought. “Magical” thinking implies the belief that performing certain rituals or actions will cause something unwanted (reminiscent of superstition).
This allows a person to feel the illusion of comfort, as if he has a huge influence on the control and events of what is happening. Most often, a person, wanting to feel calmer, constantly performs rituals, this leads to the progression of OCD.
Certain types of OCD involve the belief that everything needs to be done perfectly, that there is always perfect solution, and what sales a small mistake will have significant consequences. This is often found in patients diagnosed with OCD who strive for order, and most often in those people who suffer from anorexia nervosa.
Also very important aspect- overestimation of the danger of the situation and underestimation of the ability to cope with it. Most people who suffer from OCD believe that they must know for sure that bad things will not happen. For these people, OCD is a kind of absolute insurance. They believe that if they try hard, perform more rituals and take good insurance, they will have more certainty. In fact, trying too hard only leads to increased feelings of uncertainty and more doubt.
 Research has proven that psychotherapy significantly helps 70% of people diagnosed with OCD. There are two main ways to treat the disorder: psychotherapy and medications. However, they can be used simultaneously.
Research has proven that psychotherapy significantly helps 70% of people diagnosed with OCD. There are two main ways to treat the disorder: psychotherapy and medications. However, they can be used simultaneously.
But still not drug therapy preferable, since OCD can be easily corrected without medications. Psychotherapy has no side effects on the body and has a more lasting effect. Medicines may be prescribed as treatment when the neurosis is complicated, or as a short-term measure to relieve symptoms before starting psychiatric treatment.
For the treatment of OCD EMDR therapy is used, cognitive behavioral psychotherapy(CBT), hypnosis and strategic short-term psychotherapy.
The method of confrontation with simultaneous suppression of anxious emotions was recognized as the first effective psychological method of treating OCD. Its meaning lies in a carefully dosed confrontation with obsessive thoughts and fears, but without the typical avoidance reaction. As a result, a person gets used to it over time, and fears gradually disappear.
But not everyone has the strength to go through this treatment, so this method has been refined with CBT, which focuses on changing the response to impulses (the behavioral part), as well as changing the meaning of the intrusive urges and thoughts that arise (the cognitive part).
 Any of the above psychotherapeutic treatments for the disorder allows break the cycle of anxiety, obsessions and avoidance reactions. And it makes no difference whether you and the psychotherapist first focus on analyzing the meanings that the patient attaches to events and thoughts with further elaboration of alternative reactions to them. Or the focus is on reducing the level of discomfort from working through obsessions. Or it is the restoration of the ability to unconsciously filter obsessive thoughts before they reach the conscious level.
Any of the above psychotherapeutic treatments for the disorder allows break the cycle of anxiety, obsessions and avoidance reactions. And it makes no difference whether you and the psychotherapist first focus on analyzing the meanings that the patient attaches to events and thoughts with further elaboration of alternative reactions to them. Or the focus is on reducing the level of discomfort from working through obsessions. Or it is the restoration of the ability to unconsciously filter obsessive thoughts before they reach the conscious level.
This treatment reduces the anxiety that OCD typically causes. The therapy methods are assimilated by the person, after which his urge to act inappropriately to the situation and anxiety disappear. Obsessive compulsive disorder is not a mental illness, since it does not lead to a change in personality, it is a neurotic disorder that is reversible with proper treatment.
 Obsessive-compulsive disorder is a dysfunction of mental activity, manifested by involuntary thoughts of an obsessive nature that interfere with normal life, as well as various fears. These thoughts create anxiety, which can only be relieved by performing obsessive and tiresome activities called compulsions.
Obsessive-compulsive disorder is a dysfunction of mental activity, manifested by involuntary thoughts of an obsessive nature that interfere with normal life, as well as various fears. These thoughts create anxiety, which can only be relieved by performing obsessive and tiresome activities called compulsions.
Obsessive-compulsive disorder can be progressive or episodic, or chronic. Obsessive thoughts are ideas or inclinations that appear again and again in a stereotypical form in a person’s head. The essence of these thoughts is almost always painful, since they are either perceived as meaningless ideas or carry obscene or aggressive content.
The root causes of the disorder in question can rarely be found on the surface. Obsessive compulsive disorder OCD is characterized by compulsions (ritualistic actions) and obsessions (obsessive thoughts). The most common involuntary intrusive thoughts are:
— fear of infection (for example, viruses, microbes, from liquids, chemicals or excrement);
Signs of obsessive-compulsive disorder in children:
— wet, cracked hands (if the child suffers from compulsive hand washing);
- prolonged stay in the bathroom;
- slow completion of homework due to fear of making a mistake;
- introducing many corrections and amendments to school work;
- strange or repetitive behavior, such as constantly checking doors or taps to make sure they are closed;
- tiresome, constant questions that require reassurance, for example, “Mom, touch it, I have a fever.”
How to treat obsessive-compulsive disorder in children? Many parents want to know this. First of all, it is necessary to accurately determine whether their child suffers from obsessive-compulsive disorder or simply practices some of his own rituals. We can identify quite normal rituals for children, which parents often mistake for violations. These include:
- children under three years of age often have certain “traditions” of going to bed; by the school period this usually either goes away or becomes mild;
- invented games with certain rules, collecting (starting from the age of five);
- excessive passion for some performer, subculture, which is a way of socialization, building relationships with peers who have similar hobbies.
Before getting rid of obsessive-compulsive disorder, parents need to differentiate it from the normal manifestations inherent in age period, in which their baby is located. The main difference between the described syndrome and normal rituals is the understanding by adolescents and children of the abnormality of obsessive thoughts and ritual actions. Children realize that their actions are deviant from the norm, so they try to resist them. This understanding pushes them to hide obsessive thoughts and ritual actions from the environment. Therefore, if a baby openly performs a certain ritual before going to bed, this does not indicate the presence of an illness. You need to understand that such behavior is only inherent in his age period.
Previously, the syndrome in question was considered a condition that was resistant (unresponsive) to treatment, since traditional psychotherapeutic methods based on the principles rarely brought effect. Also, the results of using various medicines. However, in the eighties of the last century, the current situation changed dramatically due to the introduction of new methods of behavioral therapy and pharmacopoeial medicine, the effectiveness of which was proven through large-scale studies.
Scientists of that time, trying to find the answer to the question “how to treat obsessive-compulsive disorder,” experimentally proved that the most effective method behavioral therapy The disorder in question is a method of preventing reaction and exposure.
The patient receives instructions on how to resist performing compulsive actions, after which he is placed in a situation that provokes discomfort caused by obsessions.
The main thing in the treatment of the disease in question is the timely recognition of obsessive-compulsive disorder and correct diagnosis.
Currently, the main medications for the treatment of obsessive-compulsive disorder are selective serotonin reuptake inhibitors (Clomipramine), anxiolytics (Clonazepam, Buspirone), mood stabilizers (Lithium drugs) and antipsychotics (Rimozide).
How to get rid of obsessive-compulsive disorder? Most therapists agree that treatment of this disease should begin with the prescription of antidepressants, namely drugs of the group selective inhibitors serotonin reuptake in an adequate dose. Drugs of this pharmacotherapeutic group are better tolerated by patients and are considered safer than Clomipramine (a tricyclic antidepressant that blocks serotonin reuptake), previously widely used in the treatment of the disorder in question.
It is also practiced to prescribe anxiolytics in combination with other drugs. It is not recommended to use them as monotherapy. The prescription of mood stabilizers, namely Lithium preparations, is indicated, since Lithium promotes the release of serotonin.
A number of researchers have proven the effectiveness of prescribing atypical antipsychotics (Olanzapine) in combination with serotonergic antidepressants.
In addition to the use of drugs in the treatment of obsessions and compulsions modern approach involves the use of psychotherapeutic methods. An excellent psychotherapeutic effect is provided by the four-step technique, which provides the opportunity to simplify or modify ritual procedures. This method is based on the patient’s awareness of the problem and gradual overcoming of symptoms.
Treatment of obsessive compulsive disorder at home is not recommended, but there are a number of therapeutic and preventive measures that can reduce the severity of symptoms.
So, treatment for obsessive compulsive disorder at home involves:
- reducing the consumption of alcohol and drinks containing caffeine;
- getting rid of bad habits;
- regular meals, because the feeling of hunger, lack nutrients, a decrease in sugar levels can provoke a stressful condition, which will cause symptoms of obsessive-compulsive disorder;
- regular execution physical exercise, since the systematic release of endorphins improves metabolism, increases stress resistance and improves general health person;
- massage;
— establishing optimal sleep and wakefulness patterns;
- taking warm baths, during which a cool compress should be placed on the head of the suffering individual, this procedure should be carried out several times a week for twenty minutes, each procedure must reduce the temperature of the water;
- to relieve anxiety, for the purpose of relaxation and calming of a sick individual, taken orally herbal decoctions and infusions that have a sedative effect (the herbs of valerian officinalis, lemon balm, and motherwort are used);
- systematic use of St. John's wort, which allows you to increase mental concentration, improve clarity of consciousness, which affects the force of compulsion to perform ritual actions;
- daily conduct breathing exercises, which allows you to restore a normal emotional background, contributing to a “sober” assessment of the current situation.
After therapy, social rehabilitation is required. Only in case of successful adaptation after treatment of obsessive-compulsive disorder clinical symptoms will not come back. The complex of rehabilitation measures includes training in fruitful interaction with the social and immediate environment. For complete cure In case of obsessive-compulsive disorder, the support of loved ones plays a special role.
The famous German philosopher Arthur Schopenhauer argued that nine-tenths of our happiness depends on health. Without health there is no happiness! Only complete physical and mental well-being determine human health, help us successfully cope with illnesses and adversities, lead an active social life, reproduce, and achieve our goals. Human health is the key to a happy, fulfilling life. Only a person who is healthy in all respects can be truly happy and capable ofto fully experience the fullness and diversity of life, to experience the joy of communicating with the world.
They talk about cholesterol so unflatteringly that they are just right to scare children. Do not think that this is a poison that only does what destroys the body. Of course, it can be harmful and even dangerous to health. However, in some cases, cholesterol turns out to be extremely necessary for our body.
The legendary balm “star” appeared in Soviet pharmacies in the 70s of the last century. It was in many ways an irreplaceable, effective and affordable drug. “Star” tried to treat everything in the world: acute respiratory infections, insect bites, and pain of various origins.
Language is important organ a person who not only can talk incessantly, but can talk about a lot without saying anything. And I have something to tell him, especially about health.
Despite its small size, the tongue performs a number of vital functions.Over the past few decades, the prevalence allergic diseases(AZ) received epidemic status. According to the latest data, more than 600 million people worldwide suffer from allergic rhinitis(AR), approximately 25% of them are in Europe.
For many people, there is an equal sign between a bathhouse and a sauna. And very few of those who realize that the difference exists can clearly explain what this difference is.
Having examined this issue in more detail, we can say that there is a significant difference between these pairs.Late autumn, early spring, periods of thaw in winter - this is a period of frequent colds, both adults and children. From year to year the situation repeats itself: one family member falls ill and, like a chain, respiratory disease follows. viral infection they endure everything.
In some popular medical weeklies you can read odes to lard. It turns out that it has the same properties as olive oil, and therefore can be consumed without any reservations. At the same time, many argue that you can help the body “cleanse” only by fasting.
In the 21st century, thanks to vaccination, the prevalence infectious diseases. According to WHO, vaccination prevents two to three million deaths per year! But, despite the obvious benefits, immunization is shrouded in many myths, which are actively discussed in the media and in society in general.
Obsessive-compulsive disorder, also abbreviated as OCD, refers to complexes of symptoms that are grouped together and derived from the combined Latin terminology obsessio and compulsio.
Obsession itself, translated from Latin, means siege, taxation, blockade, and compulsion, translated from Latin, means coerce.
Obsessive drives, varieties of obsessive phenomena (obsessions), are characterized by unbearable and very irresistible drives that arise in the head in defiance of reason, will and feelings. Very often they are accepted by the patient as unacceptable and are contradictory to his moral and ethical principles and are never realized in comparison with the impulsive drives of compulsion. All these attractions are recognized by the patient themselves as wrong and are very difficult for them to experience. The very occurrence of these drives, by the nature of their incomprehensibility, very often contributes to the emergence of a feeling of fear in the patient.
The term compulsion itself is often used to refer to obsessions in the sphere of movements, as well as obsessive rituals.
If we turn to domestic psychiatry, we will find that obsessive states are understood as psychopathological phenomena that are characterized by the emergence in the patient’s mind of phenomena of a certain content, accompanied by a painful feeling of compulsion. Obsessive states are characterized by the emergence of involuntary, contrary to the will, obsessive desires with clear awareness. But these obsessions in themselves are alien, unnecessary in the patient’s psyche, but the sick person cannot get rid of them. The patient has a close connection with emotionality, as well as depressive reactions and a feeling of unbearable anxiety. When the above symptoms occur, it has been established that they do not affect the intellectual activity itself and, in general, are alien to his thinking, and also do not reduce its level, but worsen performance and productivity itself mental activity. Throughout the entire period of illness, a critical attitude towards the ideas of obsession is maintained. Obsessive states are preliminarily divided into intellectual-affective obsessions (phobias), as well as motor ones (compulsions). In most cases, the very structure of the disease of obsessions combines several of their types. Isolating obsessions that are abstract or indifferent in their content (affectively indifferent), for example, arrhythmomania, is often unjustified. When analyzing the psychogenesis of neurosis, it is possible to see at the basis
Obsessive-compulsive disorder - causes
The causes of obsessive-compulsive disorder are genetic factors of a psychasthenic personality, as well as intrafamily problems.
With elementary obsessions, in parallel with psychogenics, there are cryptogenic causes, in which the very reason for the occurrence of experiences is hidden. Obsessive states are observed mainly in people with a psychasthenic character, and fears of an obsessive nature, as well as these n.s., are especially important here. occur during the period of neurosis-like conditions at the time of sluggish schizophrenia, epilepsy, after traumatic brain injury and somatic diseases, with hypochondriacal-phobic or nosophobic syndrome. Some researchers believe that the clinical picture of the genesis of obsessive-compulsive disorder plays important role mental trauma, as well as conditioned reflex stimuli that have become pathogenic due to their coincidence with other stimuli that previously caused a feeling of fear. Situations that have become psychogenic due to the confrontation of opposing tendencies play an important role. But it should be noted that these same experts note that obsessive states arise when there is various features character, but still more often in psychasthenic individuals.
To date, all these obsessive states have been described and included in International Classification Diseases called obsessive-compulsive disorder.
OCD occurs very often with a large percentage of morbidity and requires urgently attracting psychiatrists to the problem. Currently, ideas about the etiology of the disease have expanded. And it is very important that the treatment of obsessive-compulsive disorder is directed towards serotonergic neurotransmission. This discovery has provided the potential for recovery for millions around the world who have obsessive-compulsive disorder. How to replenish the body with Serotonin? Tryptophan will help with this - an amino acid that is found in a single source - food. And already in the body Tryptophan is converted into Serotonin. This transformation produces mental relaxation and also creates a sense of emotional well-being. Further, Serotonin acts as a precursor to melatonin, which regulates the biological clock.
This discovery that potent serotonin reuptake inhibition (SSRI) holds the key to the most effective treatment for obsessive-compulsive disorder and was the very first step in the revolution in clinical studies, where the effectiveness of such selective inhibitors was noted
Obsessive-compulsive disorder - history
The clinic of obsessive disorders has attracted the attention of researchers since the 17th century.
They were first talked about in 1617, and in 1621 E. Barton described the obsessive fear of death. Research in the field of obsession was described by F. Pinel (1829), and I. Balinsky introduced the term “obsessive ideas,” which were included in Russian psychiatric literature. Since 1871, Westphal coined the term “agoraphobia,” which refers to the fear of being in public places.
In 1875, M. Legrand de Sol, analyzing the peculiarities of the dynamics of the course of obsessive-compulsive disorder in forms of insanity of doubts together with delusions of touch, found out that the clinical picture was gradually becoming more complex, in which obsessive doubts were replaced by fear of touching objects in environment, and also join the motor rituals that govern the lives of the sick
Obsessive-compulsive disorder in children
But only in the XIX-XX centuries. The researchers were able to more clearly characterize the clinical picture and provide an explanation of obsessive-compulsive disorder syndromes. Obsessive-compulsive disorder itself in children often occurs in adolescence or young adulthood. The very maximum clinically isolated manifestations of OCD allocated in the range of 10 - 25 years
Obsessive-compulsive disorder - symptoms
The main features of obsessive-compulsive disorder are repetitive and very intrusive thoughts (obsessive), as well as compulsive actions (rituals).
Simply put, the core of OCD is the obsession syndrome, which is a combination in the clinical picture of thoughts, feelings, fears, memories, and all this arises beyond the wishes of the patients, but still with awareness of all the pain and a very critical attitude. Understanding the unnaturalness and illogic of obsessive states, as well as ideas, patients are very powerless in trying to overcome them on their own. All obsessive impulses, as well as ideas, are accepted as alien to the person and as if originating from within. In patients, obsessive actions are the performance of rituals that act as a relief from anxiety (this could be washing hands, wearing a gauze bandage, frequent change linen to prevent infection). All attempts to drive away uninvited thoughts and urges lead to severe internal struggle, which is accompanied by intense anxiety. These obsessive states are included in the group of neurotic disorders.
The prevalence of OCD among the population is very high. Those suffering from obsessive-compulsive disorder account for 1% of patients treated in psychiatric hospitals. It is believed that men and women get sick to the same extent.
Obsessive-compulsive disorder is characterized by the occurrence of thoughts of an obsessive, painful nature for independent reasons, but presented to the patient as their personal beliefs, ideas, and images. These thoughts forcibly penetrate into the patient’s consciousness in a stereotypical form, but at the same time he tries to resist them.
This is the union inner feeling compulsive beliefs, as well as efforts to resist them, indicate the presence of obsessive symptoms. Thoughts of an obsessive nature can also take the form of individual words, poetic lines, and phrases. For the sufferer, they can be indecent, shocking, and even blasphemous.
The obsessive images themselves are very vividly imagined scenes, often of a violent nature, as well as disgusting(sexual perversion).
Obsessive impulses
involve inducements to commit actions that are usually destructive or dangerous, or that may cause disgrace. For example, shouting obscene words in public, or jumping out sharply in front of a moving car.Obsessive rituals include repetitive activities such as counting, repeating certain words, repeating often meaningless actions such as washing hands up to twenty times, and some may develop obsessive thoughts about impending infection. Some rituals of patients include constant ordering in the laying out of clothes, taking into account complex system. One part of the patients experiences an irresistible and wild urge to carry out actions a certain number of times, and if this does not happen, then the sick are forced to repeat everything all over again. The patients themselves recognize the illogicality of their rituals and deliberately try to hide this fact. Sufferers worry and consider their symptoms a sign of incipient madness. All these obsessive thoughts, as well as rituals, contribute to the emergence of problems in Everyday life.
Obsessive rumination or simply mental chewing gum, akin to internal debates in which all the arguments for and against, including very simple everyday actions, are constantly reviewed. Some obsessive doubts relate to actions that could presumably be performed incorrectly and also not completed, for example (turning off the tap of a gas stove, as well as locking the door; and others relate to actions that could possibly cause harm to other individuals (presumably driving past hit a cyclist with a car.) Very often doubts are caused by religious precepts and rituals, namely by remorse.
As for compulsive actions, they are characterized by frequently repeated stereotypical actions that have acquired the character of protective rituals.
Along with this, obsessive-compulsive disorders distinguish a number of clear symptom complexes, including contrasting obsessions, obsessive doubts, as well as phobias ( obsessive fears).
Obsessive thoughts themselves, as well as compulsive rituals, can intensify in some situations, namely, the nature of obsessive thoughts about harming other people very often intensifies in the kitchen or somewhere in other places where there are sharp objects. Patients themselves often try to avoid such situations and there may be similarities with anxiety-phobic disorder. Anxiety itself is a significant component of obsessive-compulsive disorder. Some rituals reduce anxiety, while after other rituals it increases.
Obsessions tend to intensify as part of depression. In some patients, the symptoms resemble a psychologically understandable reaction to obsessive-compulsive symptoms, while in others there are repeated episodes depressive disorders arising due to independent reasons.
Obsessive states (obsessions) are divided into sensual or figurative, which are characterized by the development of painful affect, as well as obsessive states of affectively neutral content.
Obsessive states of the sensory plane include an obsessive feeling of antipathy, actions, doubts, intrusive memories, ideas, desires, fears about habitual actions.
Obsessive doubts include uncertainty that arose despite sound logic and reason. The patient begins to doubt the correctness of the decisions made, as well as the actions taken and completed. The very content of these doubts is different: fears about a locked door, closed taps, closed windows, turned off electricity, turned off gas; official doubts about a correctly written document, addresses on business papers, whether the numbers are indicated accurately. And despite repeated checking of the committed action, obsessive doubts do not disappear, but only cause psychological discomfort.
Intrusive memories include persistent and irresistible sad memories of unpleasant and shameful events, which are accompanied by a feeling of remorse and shame. These memories predominate in the patient’s consciousness, and this despite the fact that the patient tries to distract himself from them in any way.
Obsessive urges push to carry out a harsh or very dangerous action. At the same time, the patient experiences a feeling of fear, horror and confusion about the inability to free himself from it. The sick person has a wild desire to throw himself in front of a train, as well as to push him under a train loved one or kill his wife and child in a cruel way. The sick suffer greatly and worry about the implementation of these actions.
Obsessive ideas also appear in various options. In some cases, a vivid vision of precisely the results of the obsessive desires themselves is possible. At this moment, patients vividly imagine the vision of the cruel act they committed. In other cases, these obsessive ideas appear as something implausible, even as absurd situations, but the sick people accept them as real. For example, the faith and conviction of the sick person that the buried relative was buried while still alive. At the peak of obsessive ideas, awareness of their absurdity, as well as the implausibility itself, disappears and an acute confidence in their reality prevails.
An obsessive feeling of antipathy, this also includes obsessive blasphemous thoughts, as well as antipathy towards loved ones, unworthy thoughts towards respected people, towards saints, as well as church ministers.
Obsessive actions are characterized by actions that are committed against the wishes of the sick and despite all the restraining efforts made for them. Some of the obsessive actions burden the patient himself and this continues until they are realized.
And other obsessions pass by the patient himself. Obsessive actions are most painful when others pay attention to them.
Obsessive fear or phobias include fear of large streets, fear of heights, confined or open spaces, fear of large crowds, fear of sudden death, and fear of contracting an incurable disease. And some patients develop phobias with fear of everything (panphobia). And finally, obsessive fear (phobophobia) may occur.
Nosophobia or hypochondriacal phobias are associated with an obsessive fear of any serious illness. Stroke-, cardio-, AIDS-phobia, syphilophobia, phobia are very often noticed malignant tumors. At the very peak of anxiety, sick people often lose their critical attitude towards their health and often resort to doctors for examination and treatment of non-existent diseases.
Specific or isolated phobias include obsessive fears caused by specific situation(fear of heights, thunderstorms, nausea, pets, dental treatment, etc.). Patients experiencing fear typically avoid these situations.
Obsessive fears are often supported by the development of rituals - actions that are involved in magical spells. Rituals are performed for the reason of protection from imaginary misfortune. Rituals may include snapping fingers, repeating certain phrases, singing a tune, etc. In such cases, loved ones themselves are not at all aware of the existence of such disorders in relatives.
Obsessions of an affectively-neutral nature include obsessive philosophizing, as well as obsessive counting or remembering of neutral events, formulations, terms, etc. These obsessions weigh on the patient and interfere with his intellectual activity.
Contrasting obsessions or aggressive obsessions include blasphemous as well as blasphemous thoughts, obsessions are filled with fear of fear of harm not only to oneself, but also to others.
Patients with contrasting obsessions are troubled by irresistible desires to shout out contradictory morals cynical words, they are capable of committing dangerous and also absurd actions in the form of causing injury to themselves, as well as to their loved ones. Obsessions often go together with phobias of objects. For example, fear of sharp objects (knives, forks, axes, etc.). This group of contrasting obsessions includes sexual obsessions (the desire for perverted sexual acts with children and animals).
Misophobia- obsessions with pollution (fear of contamination with soil, urine, dust, feces), small objects (shards of glass, needles, specific types of dust, microorganisms); fear of harmful and toxic substances (fertilizers, cement, toxic waste) entering the body.
In many cases, the fear of contamination itself may be limited in nature, manifesting itself only, for example, in personal hygiene (very frequent changing of linen, repeated hand washing) or household issues (food processing, frequent mopping of floors, ban on pets). Of course, such monophobias do not affect the quality of life; they are perceived by others as personal habits of cleanliness. Clinically recurring variants of these phobias are classified as severe obsessions. They consist of cleaning things, as well as a certain sequence using detergents and towels to maintain sterility in the bathroom. Outside the apartment, the sick person implements protective measures. Appears on the street only in special and maximum covered clothing. For more later stages disease, patients themselves avoid pollution, and are even afraid to go outside and do not leave their own apartments.
One of the places among obsessions was occupied by obsessive actions, as isolated, monosymptomatic movement disorders. In childhood, these include tics. People with tics are able to shake their heads, as if checking to see if my hat fits well, make movements with their hands, as if throwing away interfering hair, and constantly blink their eyes. Along with obsessive tics, actions such as lip biting, spitting, etc. are observed.
Obsessive-compulsive disorder - treatment
As noted earlier, cases of complete recovery are relatively rare, but stabilization of the condition is possible, as well as mitigation of symptoms. Mild forms of obsessive-compulsive disorder are favorably treated on an outpatient basis, and the reverse development of the disease occurs no earlier than 1 year from the date of treatment.
And more severe forms of obsessive-compulsive disorder (phobias of contamination, sharp objects, pollution, contrasting images or numerous rituals) become more resistant to treatment.
Obsessive-compulsive disorder is very difficult to distinguish from schizophrenia, as well as Tourette's syndrome.
Schizophrenia also interferes with the diagnosis of obsessive-compulsive disorder, so to rule out these diseases you need to consult a psychiatrist.
For effective treatment Obsessive-compulsive disorder requires removal of stressful events and pharmacological intervention targeting serotonergic neurotransmission. Unfortunately, science is powerless to permanently cure this mental illness, but many specialists use a method to stop thoughts.
A reliable method of treatment for OCD is drug therapy. You should refrain from self-medication, and a visit to a psychiatrist should not be postponed.
Those suffering from obsessions often involve family members in their rituals. In this situation, relatives should treat the sick person firmly, but also sympathetically, mitigating the symptoms if possible.
Drug therapy in the treatment of obsessive-compulsive disorder includes serotonergic antidepressants, anxiolytics, minor antipsychotics, MAO inhibitors, beta blockers to stop vegetative manifestations, as well as triazole benzodiazepines. But the main ones in the treatment regimen for obsessive-compulsive disorder are atypical antipsychotics - quetiapine, risperidone, olanzapine in combination with SSRI antidepressants or antidepressants such as moclobemide, tianeptine, as well as benzodiazepine derivatives (these are alprazolam, bromazepam, clonazepam).
One of the main tasks in the treatment of obsessive-compulsive disorder is establishing cooperation with the patient. It is important to instill in the patient faith in recovery and overcome prejudices against the harm of psychotropic drugs. Support from relatives is required for the likelihood of healing of the patient
Obsessive-compulsive disorder - rehabilitation
Social rehabilitation includes building family relationships, learning how to interact properly with other people, vocational training, and teaching skills for everyday life. Psychotherapy is aimed at gaining faith in one’s strengths, self-love, and mastering ways to solve everyday problems.
Obsessive-compulsive disorder is often prone to recurrence, and this in turn requires longitudinal preventive medication.

Dream interpretation is an ancient art that allows you to at least assess the psychological status of a person, because...

As soon as the first mirrors were born, people immediately endowed them with all sorts of mystical abilities....

Photo: Anatoly ZHDANOV Understanding the program “The East is a delicate matter” on Radio “Komsomolskaya Pravda” [audio] Juma:...

Interpretation of the dream in the dream book: A man sees how he is being released from prison - the criminal sees great difficulties in life...

Making a new friend in a dream foreshadows the birth of a child. Seeing friends who have been absent for a long time - for the upcoming...

In the context of the implementation of the Federal State Educational Standard, it is of great importance. Over the course of decades, educational institutions have developed a system of work...

The manual discusses programs of domestic and foreign authors that are used in the work...

How often do we see this monster with goat horns when we lay out Tarot cards. "Devil" is the personification of hell...

Navigation: Description and history of the map: To the side of the road there is a large oak tree, in its foliage they find both shelter and food...
Dear forum visitors, I am opening this topic for fans of Patrick Walesa's "Deviant Tarot" deck...
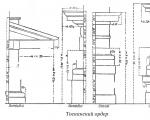
Tuscan order. Tuscan order, one of the five Roman architectural orders. The name is associated with...

LIBRETTO. If you love music (which you undoubtedly do, since you needed this book), then you'll probably...

Religion: paganism Birth: 942 (0942) Death: March on the Dnieper Family: Rurikovich Father:...

Masaccio (actually Tommaso di Giovanni di Simone Cassai (Guidi), Tommaso di ser Giovanni di Guidi; December 21...

As soon as the first mirrors were born, people immediately endowed them with all sorts of mystical abilities....

Photo: Anatoly ZHDANOV We understand the program “The East is a delicate matter” on Radio “Komsomolskaya Pravda” [audio]...