Treatment of acute heart failure is the responsibility of cardiologists. Specialists prescribe the necessary treatment course:
Prevention of acute heart failure is important. Emotional experiences, intense sports, and fast running are contraindicated for patients with heart disease. Required special diet, weight control. You should completely eliminate tobacco and alcoholic beverages from your life. The patient is able to prevent complications of this severe cardiac pathology.
Emergency measures for acute heart failure can save a person's life, since it is under serious threat. Every healthy man should know what AHF is and understand well the danger of this serious disease.
If acute heart failure occurs, the patient requires emergency care immediately. The patient’s quality of life will significantly improve as a result of timely and adequate treatment.
Various tablets for acute heart failure can be used at its initial stage, depending on its severity:
When there are symptoms of acute heart failure, and conservative treatment due to the characteristics of the diseases that caused it turns out to be ineffective, then the only option left is emergency surgery. In this case, the following may apply:
Patients with AHF stay in the hospital for an average of 10-14 days.
After stabilization of the patient's condition, the next stage of therapy is the prescription of ACE inhibitors and angiotensin-sensitive receptor blockers, mineralcorticoid receptor antagonists, and beta-blockers. If the contractility of the heart decreases (according to Echo-CG, the ejection fraction is less than 40%), then digoxin is prescribed.
When the acute period of heart failure has been overcome, a stable regimen of using diuretics has been found for at least two days, clinical recommendations for acute heart failure are as follows:
Glucose, which honey is rich in, is an energy material needed by the heart muscle. However, when honey is used in excessive quantities, and even with hot tea, the heart begins to work energetically, and increased sweating occurs. There is no need to put such additional strain on a sick heart.
Therefore, for heart failure, folk remedies such as honey should be consumed in small doses up to 3 times a day, 1 teaspoon or 1 tbsp. spoon, with fruit, cottage cheese, milk, etc. Remember that at temperatures above 60°C, honey loses its beneficial properties!
One of the treatments for acute heart failure with folk remedies is treatment with leeches. Such procedures are carried out up to 2 times a week. The peculiarity of these procedures is that patients suffering from heart failure are subject to long-term treatment.
If the development of the disease occurs with venous congestion, enlarged liver, congestive wheezing in the lungs, leeches in this case are applied for the maximum period until they disappear on their own. If decompensation is present, then the main areas for installing leeches are the sacral and hepatic zones.
In order to improve the functioning and condition of the heart muscle, leeches are placed on local points located in the cardiac zone. Zones are selected depending on clinical indications and the body’s reaction to the procedure. The course of treatment is usually 7 - 12 procedures.
For one procedure – 4-8 attachments. If the patient's condition is relatively satisfactory, the number is reduced to 3-4 leeches per procedure, and the course of treatment is extended.

Phytoncides contained in the leaves of trees and shrubs have a beneficial effect on the cardiovascular system. So for people suffering from heart failure, to stimulate the cardiovascular system, it is useful to walk as often as possible under poplars, eucalyptus or laurels, near flowering lilac and hawthorn bushes.
And you can plant a lemon in your apartment. Its phytoncides not only have beneficial effect on the cardiovascular system, but also have a tonic effect on the entire body. It is recommended to regularly chew lemon peel to improve heart function.
As is known from the treatises of ancient Indian medicine, small doses of cardamom added to tea or vegetables stimulate the heart. Eating viburnum berries, both fresh and frozen, has a beneficial effect on the heart and reduces blood pressure in hypertension.
- Recipe. Viburnum berries are a folk remedy for acute heart failure.
Take a glass of viburnum, fill it with hot water (liter) and cook for 8-10 minutes. Add 3 tbsp honey to the strained viburnum decoction. spoons. Take half a glass up to 4 times a day.
- Recipe. Garlic as a rub for swollen legs in acute heart failure.
If your legs swell due to heart failure, you should definitely rub them morning and evening. Grind the garlic into a paste. Pour water (2 glasses) into a spoonful of this paste and boil for 5 minutes. Rub the cooled, strained garlic mixture onto your feet.
- Recipe. Parsley as a remedy for edema in acute heart failure.
Grind the parsley (roots along with herbs) in a meat grinder in such an amount that the output is 1 cup of gruel.
Pour it into a glass or enamel container with 2 glasses of boiling water, close it and leave to infuse for 8-9 hours in a warm place. After this, squeeze out the mass, and add lemon juice squeezed from a medium-sized lemon to the strained infusion.
Take 1/3 cup for 2 days, after a three-day break, resume taking it and drink for another two days.
- Recipe. Strengthening the heart muscle with a mixture of dried apricots, raisins, nuts, lemon and honey for acute heart failure.
The components of the recipe contain everything that a weakened heart muscle needs. Dried apricots, raisins and nuts, in addition to vitamins and microelements, are rich in potassium, which she needs so much. Prepared in October-November.
Buy 300g of raisins (preferably the so-called “cordial” ones) of blue color), dried apricots (to your taste), walnut kernels, honey and lemons. Wash and dry dried fruits. Grind all the ingredients (except honey) by passing them through a meat grinder (lemons along with the peel).
Add honey to the resulting slurry and mix well. Transfer the medicine into clean jars and place in a cool place. Take 1 tbsp daily, up to 3 times a day with meals. spoon until the medicine runs out.
Prevention


Carrying out a comprehensive examination, the task of which is to identify the risk of malignant ventricular arrhythmia and sudden cardiac arrest, allows for timely adoption of adequate therapeutic measures.
Prevention of sudden death is based on the influence on risk factors:
- myocardial ischemia;
- threatening arrhythmia;
- weakening of the contractility of the left ventricle.
Numerous experiments have revealed the effectiveness of beta-adrenergic receptor blockers in preventing sudden cardiac arrest in patients who have had a heart attack. The effectiveness of such drugs is due to their antiarrhythmic and bradycardic effect.
Currently, treatment with beta-blockers is indicated for all post-infarction patients who have no contraindications. It is preferable to take cardioselective drugs that do not have sympathomimetic activity.
Treatment with beta-blockers minimizes the risk of sudden cardiac arrest not only in people suffering from coronary artery disease, but also hypertension. Treatment with the calcium antagonist verapamil in patients who have had a heart attack and do not have signs of heart failure contributes to a reduction in mortality.
This drug is similar in action to beta-blockers. Risk reduction sudden death can be achieved through primary prevention myocardial ischemia, i.e., a complex effect on the main risk factors:
- smoking;
- high blood pressure;
- high cholesterol, etc.
The effectiveness of anti-sclerotic drugs from the class of statins has been proven. Patients with life-threatening arrhythmia that cannot be treated with medication undergo surgical treatment:
- introduction of pacemakers for bradyarrhythmia;
- sewing in defibrillators for tachyarrhythmia and recurrent ventricular fibrillation;
- intersection of pathologically altered pathways in the syndrome premature arousal ventricles;
- elimination of arrhythmogenic foci in the heart muscle.
Despite the advances of modern medicine, it is not always possible to identify a potential victim of sudden cardiac death. If installed high risk sudden cessation blood circulation, it is also not always possible to prevent it.
Based on this, the most important aspect of the fight against fatal arrhythmia is the timely implementation of resuscitation measures during developing circulatory arrest. It is important that not only medical workers, but the majority of citizens knew the basics of resuscitation care.
- Regular observation (examination at least 2 times a year) by a specialist in the presence of chronic diseases of the cardiovascular system, timely treatment for medical care and accurate implementation of recommendations.
- Most effective prevention diseases of the cardiovascular system is to reduce the adverse effects of threat factors:
- quitting smoking and overuse alcohol (for men, the permissible dose is no more than 30 g of alcohol per day);
- elimination of psycho-emotional overloads;
- maintaining optimal body weight (for this, the body mass index is calculated: weight (in kilograms) divided by squared height (in meters), the normal figure is 20-25).
Regular physical activity: - daily dynamic cardio training - brisk walking, running, swimming, skiing, cycling and more;
- each lesson lasts 25-40 minutes (warm-up (5 minutes), main part (15-30 minutes) and final period (5 minutes), when the pace of physical exercise gradually slows down);
- It is not recommended to exercise within 2 hours after eating; After finishing classes, it is also advisable not to eat for 20-30 minutes.
Blood pressure control. Rational and balanced diet(eating foods high in fiber (vegetables, fruits, greens), avoiding fried, canned, too hot and spicy foods). Control of cholesterol levels (a fat-like substance that is a “building material” for body cells).
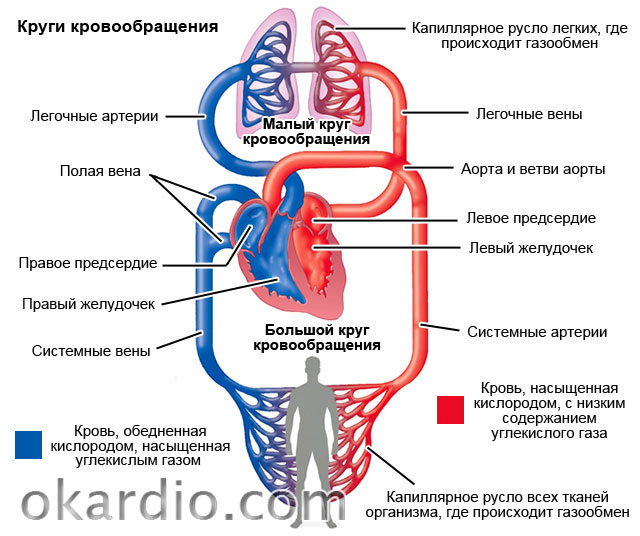
- Pathogenesis of acute heart failure (left ventricular form)
- Pathogenesis of acute heart failure (right ventricular type)
- Primary and secondary causes of acute heart failure
- Acute heart failure: causes and classification
Due to circulatory problems in the heart, it develops; the reasons why it can occur are quite extensive. WITH medical point vision, acute heart failure is not regarded as a disease - it is a consequence of past illnesses.
The heart is not able to pump the volume of blood that is necessary for the balanced functioning of the entire body. It should be noted that almost every disease of the cardiovascular system can cause this syndrome. Acute insufficiency can also occur due to frequent nervous overstrain, or may be a consequence of constant stressful situations or depression. 82% of overweight people suffer from heart failure.
Pathogenesis of acute heart failure (left ventricular form)
This type is much more common than the right ventricular form. Due to the influence of various factors, the contractility of the left ventricle is reduced, while the function of the right ventricle can be preserved.
 In this case, the pulmonary vessels become overfilled with blood, and accordingly, the pressure in the arteries increases (pulmonary circulation), which begins the process of plasma leakage through the walls of the vessels. Due to pathological changes, gas exchange and the balance of oxygen in the blood and tissues are disrupted, and, as a result, respiratory failure. Accordingly, a large number of substances are released, such as:
In this case, the pulmonary vessels become overfilled with blood, and accordingly, the pressure in the arteries increases (pulmonary circulation), which begins the process of plasma leakage through the walls of the vessels. Due to pathological changes, gas exchange and the balance of oxygen in the blood and tissues are disrupted, and, as a result, respiratory failure. Accordingly, a large number of substances are released, such as:
- adrenalin;
- norepinephrine;
- biologically active substances.
All these processes lead to the fact that the vessels become permeable, peripheral resistance increases, and this is a direct path to pulmonary edema.
Return to contents
Pathogenesis of acute heart failure (right ventricular type)
 Right ventricular acute heart failure can develop when there is an excess supply of fluid, that is, the ventricle is simply overloaded. The reasons for this may be thromboembolism, embolism, rapid blood transfusion, blood replacement fluids. Especially in cases where the catheter is inserted into the subclavian or jugular vein.
Right ventricular acute heart failure can develop when there is an excess supply of fluid, that is, the ventricle is simply overloaded. The reasons for this may be thromboembolism, embolism, rapid blood transfusion, blood replacement fluids. Especially in cases where the catheter is inserted into the subclavian or jugular vein.
The thromboembolic form can occur when blood clots form in the veins of the legs ( varicose veins veins), attacks of atrial fibrillation, smoking, prolonged standing in one position, increased blood clotting. All of these processes cause increased blood viscosity and the formation of blood clots, which interfere with normal blood flow and contribute to overload of the right ventricle.
Return to contents
Primary and secondary causes of acute heart failure
One of the main and main reasons for the development of the disease is impaired contractile function of the myocardium. The causes can be classified into two groups: they can be primary or secondary. But such a classification can be called conditional. Almost always, acute failure occurs due to a mixed type of cause.
The primary causes of the development of the disease are: acute infectious diseases, exposure to toxic poisons on the body during poisoning.
 No wonder doctors believe that infectious diseases cannot be carried “on your feet”, because they cause complications on the heart. Some of the primary causes of acute failure are the consequences of influenza, rheumatism, measles, scarlet fever, transferred to childhood, hepatitis A, typhoid fever, acute respiratory viral infections, especially in the case of severe forms and the occurrence of sepsis. All listed diseases contribute to the formation of acute inflammation, which, in turn, leads to the development of cell dystrophy, oxygen exchange is disrupted and hypoxia (oxygen starvation) occurs, and there is a lack of nutrients in cells and tissues. Impaired nervous regulation affects the heart muscle, which leads to deterioration of its condition or dystrophy. The causes of acute failure can be severe strokes, their consequences, renal pathologies, alcohol, nicotine, narcotic drugs and medications (especially in overdose), anemia, diabetes.
No wonder doctors believe that infectious diseases cannot be carried “on your feet”, because they cause complications on the heart. Some of the primary causes of acute failure are the consequences of influenza, rheumatism, measles, scarlet fever, transferred to childhood, hepatitis A, typhoid fever, acute respiratory viral infections, especially in the case of severe forms and the occurrence of sepsis. All listed diseases contribute to the formation of acute inflammation, which, in turn, leads to the development of cell dystrophy, oxygen exchange is disrupted and hypoxia (oxygen starvation) occurs, and there is a lack of nutrients in cells and tissues. Impaired nervous regulation affects the heart muscle, which leads to deterioration of its condition or dystrophy. The causes of acute failure can be severe strokes, their consequences, renal pathologies, alcohol, nicotine, narcotic drugs and medications (especially in overdose), anemia, diabetes.
Secondary ones do not have a direct effect on the myocardium. That is, it occurs due to overwork and oxygen starvation. Such disorders can occur against the background of a hypertensive crisis, tachycardia, arrhythmia (paroxysmal diseases associated with rhythm imbalance), atherosclerotic damage to the coronary vessels. The cause of acute heart failure can be the herpes virus, cytomegalovirus, which damage the coronary vessels.
If a person, for example, has hypertonic disease, then the heart muscle works with increased vascular resistance. The myocardium increases in size - its thickness reaches 3 cm, although normally it should be no more than 14 mm. The weight of the heart also increases to 0.5 kg (normal 385 g). It is very difficult for the vessels to supply the required volume of blood to the enlarged heart muscle. Due to the fact that there is a pathological change and a violation of the ability to contract, during an attack of hypertension, heart failure occurs.
Return to contents
Acute heart failure: causes and classification
 The causes of this disease can be classified by dividing them into the following groups:
The causes of this disease can be classified by dividing them into the following groups:
- through which myocardial damage occurs;
- for which the heart is overloaded;
- causing rhythm disturbances;
- which lead to the heart overflowing with blood.
Acute heart failure can occur when the causes are destructive and myocardial damage occurs. This can occur against the background of myocarditis ( infectious inflammation muscles), cardiomyopathy (myocardial damage caused by non-inflammatory processes and tumors), myocardial infarction (thrombosis coronary artery), angina pectoris (a form of coronary artery disease), cardiosclerosis (damage to valves and muscles due to the development of scar tissue in them). Allergic tissue damage caused by bronchial asthma and Lyell's syndrome can cause destruction of the myocardium. With systemic connective tissue diseases (against the background of lupus or rheumatism), acute circulatory failure may develop.
It can also occur due to cardiac overload. In such cases, the heart either pumps larger volumes of blood or works with greater resistance from the blood vessels. Acute failure due to overload may appear as a result of stenosis of the aorta or pulmonary trunk (a barrier is created to the exit of blood flow from the heart), arterial hypertension (increased pressure in the arteries), pulmonary hypertension (sharply increased intravascular pressure in the blood flow of the pulmonary arteries), pathological changes valve apparatus (develops with congenital and acquired defects).
 Abnormal heart rate can be considered a cause of acute heart failure. An abnormal heart rate occurs if electrolyte balance, urea and creatinine levels, so contractions simply become ineffective. The cause of rhythm failure can be atrial fibrillation, tachycardia, or bradyarrhythmia.
Abnormal heart rate can be considered a cause of acute heart failure. An abnormal heart rate occurs if electrolyte balance, urea and creatinine levels, so contractions simply become ineffective. The cause of rhythm failure can be atrial fibrillation, tachycardia, or bradyarrhythmia.
Acute failure can occur as a consequence of an altered process of filling the heart with blood. The etiology is external compression of the heart walls or due to their rigidity. Such obstacles prevent the heart from filling with sufficient blood, which leads to pathological changes in blood pumping and blood circulation in general. The causes of acute failure in such pathological changes are pericarditis (inflammation of the outer protective membrane of the heart - the pericardium), cardiac tamponade (pathological changes in cardiac hypodynamics). Heart failure develops from stenosis of the atrioventricular valves (narrowing of the atrioventricular opening), amyloidosis, fibroelastosis (increased stiffness of the heart walls).
In childhood (up to 3 years), the causes of acute failure can be: congenital heart disease, myocarditis, complications after infectious diseases. In adolescents, acute heart failure occurs more often due to the use of narcotic drugs and smoking.
Acute heart failure should be treated only in a hospital setting; self-medication should never be done; the disease can cause fluid accumulation in the respiratory tract, slow blood flow, which will lead to cerebral hypoxia and kidney dysfunction. In many cases, if treated negligently, acute heart failure causes death.

Description:
Acute (AHF) is a clinical syndrome characterized by the rapid onset of symptoms characteristic of impaired cardiac function (reduced cardiac output, insufficient tissue perfusion, increased pressure in the capillaries of the lungs, tissue congestion). It develops without connection with the presence of cardiac pathology in the past. Cardiac disorders may be systolic or diastolic dysfunction, cardiac arrhythmias, preload and afterload disorders. These violations are often life-threatening and require emergency measures. AHF may develop as acute illness de novo (that is, in a patient without pre-existing cardiac dysfunction) or as acute decompensation.
Symptoms:
Complaints. Upon admission, the patient complains of shortness of breath / suffocation, dryness, hemoptysis, fear of death. With the development of pulmonary edema, a cough appears with foamy sputum, often pink in color. The patient takes a forced sitting position.
During a physical examination, special attention should be paid to palpation and auscultation of the heart, determining the quality of heart sounds, the presence of III and IV sounds, the presence and nature of murmurs. In elderly patients, it is necessary to determine signs of peripheral: uneven pulse, murmurs in the carotid arteries and abdominal aorta. It is important to systematically evaluate the state of peripheral circulation, skin temperature, and the degree of filling of the ventricles of the heart. Right ventricular filling pressure can be assessed using venous pressure measured in the external jugular or superior vena cava. Increased left ventricular filling pressure is usually indicated by the presence of moist rales on auscultation of the lungs and/or signs of pulmonary congestion on chest examination.
ECG. In acute heart failure, the ECG is extremely rarely unchanged. Determining the rhythm and signs of overload can help identify the etiology of AHF. Of particular importance is the registration of an ECG if there is a suspicion of. In addition, the ECG can reveal the load on the left or right ventricle, atria, signs of perimyocarditis and chronic diseases such as ventricular hypertrophy or dilatation.
Killip classification
Stage I - no signs of heart failure.
Stage II - heart failure (moist rales in the lower half of the lung fields, III tone, signs of venous hypertension in the lungs).
Stage III - severe heart failure (overt; rales extending to more than the lower half of the lung fields).
Stage IV - (systolic blood pressure less than 90 mm Hg with signs of peripheral vasoconstriction: oliguria, cyanosis, sweating).
AHF is characterized by a variety of clinical variants:
- pulmonary edema (confirmed by chest X-ray) - severe respiratory distress with rales in the lungs, orthopnea and usually arterial oxygen saturation - cardiogenic shock - a clinical syndrome characterized by tissue hypoperfusion due to heart failure that persists after correction preload. Regarding hemodynamic parameters, there are no clear definitions of this condition. Arterial hypotension is usually observed (systolic blood pressure 60 beats/min; tissue congestion is possible, but not necessary;
- acute decompensated heart failure (first-time decompensation of CHF) with characteristic complaints and symptoms of moderate AHF that do not meet the criteria for cardiogenic shock, pulmonary edema or;
- hypertensive AHF - symptoms of AHF in patients with relatively preserved left ventricular function in combination with high blood pressure and an x-ray picture of venous congestion in the lungs or pulmonary edema;
- heart failure with high cardiac output - symptoms of AHF in patients with high cardiac output, usually in combination with tachycardia (due to arrhythmias, thyrotoxicosis, Paget's disease, iatrogenic and other causes), warm skin and extremities, pulmonary congestion and sometimes low blood pressure (septic shock);
- right ventricular failure - low cardiac output syndrome in combination with increased pressure in the jugular veins, liver enlargement and arterial hypotension.
Causes:
The main causes and factors contributing to the development of AHF:
1. Decompensation of chronic heart failure.
2. Exacerbation of coronary artery disease (acute coronary syndrome):
- myocardial infarction or unstable with widespread myocardial ischemia;
- mechanical complications;
- right ventricular myocardial infarction.
3. Hypertensive crisis.
4. Acutely arisen.
5. Acutely occurring valvular regurgitation, aggravation of previous valvular regurgitation.
6. Severe aortic stenosis.
7. Heavy spicy.
8. .
9. Aortic dissection.
10. Postpartum cardiomyopathy.
11. Non-cardiac provoking factors:
- insufficient adherence to treatment;
- volume overload;
- infections, especially and;
- heavy ;
- extensive surgery;
-
It must also be remembered that nitroglycerin (or its analogues) also helps to reduce blood pressure tension in the blood vessels. Therefore, the patient should be given (under the tongue!) a nitroglycerin tablet or one drop of its one percent solution (available in pharmacies). In especially severe cases, you can temporarily (until the doctor arrives) apply tourniquets to the thigh area to exclude a certain amount of blood from circulation. Tourniquets should be applied 5-10 minutes after the patient is transferred to a semi-sitting (sitting) position, since the movement of blood to the lower parts of the body does not occur instantly. If you know how to administer the medicine intravenously, immediately administer 0.3-0.5 ml of a 0.05% solution of strophanthin with 20 ml of sterile physiological solution.
Most often, HF is associated with a violation of the heart’s ability to pump blood through the vessels; therefore, the direct causes of the disease can be considered various heart defects, coronary disease, as well as arterial hypertension- in women, it is the latter that most often causes heart failure, while in men the root cause is often ischemia.
Additional factors that increase the chances of heart failure are myocarditis, diabetes mellitus, regular smoking/alcohol consumption, and cardiomyopathies. Cardiosclerosis and other designated causes of heart failure also provoke the development of cardiac asthma, which is very dangerous for older people and often causes their death even before development last stage SN.

Often, heart failure in people is detected very late, sometimes already in the terminal stage. This is due to the vagueness and ambiguity of the symptoms of the disease in the early stages of its development - it is for this reason that people who have experienced myocardial infarction or have chronic problems with the cardiovascular system are regularly asked to undergo medical examinations, since only a comprehensive diagnosis is the most effective method early detection Problems.
Manifestations of heart failure
The visible symptoms of heart failure directly depend on the location of the problem. So, in case of problems with the left ventricle, the patient is diagnosed with dry wheezing, shortness of breath, hemoptysis, and cyanosis. In case of right ventricular insufficiency, the patient complains of swelling in the extremities, as well as pain in the right hypochondrium, which indicates problems with liver function due to excess venous blood in this body.
In addition, regardless of the location of the problem, one of the typical characteristic signs of HF can be considered rapid fatigue and decreased ability to work.
Stages of the disease

The basic classification of symptoms by stages of development and severity includes five stages:
- Palpitations also appear during strong physical activity, which had not previously provoked physiological fatigue. The ability to work is practically not reduced, the functions of organs are not impaired.
- Long-term insufficiency and hemodynamic disturbances during moderate and light physical activity.
- Similar to the second one, but with visible additional pathogenic symptoms- dry cough, interruptions in heart function, congestion in the pulmonary and systemic circulation, low-grade swelling of the extremities, slight enlargement of the liver. In this case, working capacity is significantly reduced.
- Severe shortness of breath even in a state of complete rest, severe cyanosis, constant swelling, ascites, severe forms of oliguria, signs of the onset of liver cirrhosis, congestive changes in the lungs. In this state, a person is unable to work.
- Final dystrophic stage. Multiple hemodynamic disturbances, disturbance metabolic processes, morphological changes in organ groups, physical exhaustion and disability. Conservative treatment in this case is not effective.
Classification by localization
- In the left ventricle. It is formed when this part of the heart is overloaded, its contractile function is reduced, the aorta narrows, or the myocardium malfunctions.
- In the right ventricle. Stagnation of blood in the systemic circulation and insufficient supply of the small one. It is most often diagnosed with pulmonary hypertension.
- In both ventricles. Mixed type with additional complications.
Classification by origin
- Overload - develops with heart defects and problems associated with systemic circulatory disorders.
- Myocardial - damage to the walls of the heart with disruption of muscle energy exchange.
- Mixed - combines increased load and myocardial damage.
Forms
Doctors divide heart failure into two main forms:
Acute heart failure
This type of heart failure develops rapidly, often within 1–2 hours. The main causes are mitral/aortic valve insufficiency, myocardial infarction, or rupture of the walls of the left ventricle. Basic manifestations include cardiogenic shock, cardiac asthma, and pulmonary edema.
Chronic heart failure
Develops gradually, can form throughout long period time, flesh up to several years. Clinical manifestations in this case, they are similar to acute heart failure, but the treatment process itself is longer, and with severe stages The disease is still not effective. Basic reasons chronic HF - heart defects, long-term anemia, arterial hypertension, generalized chronic respiratory failure in the decompensation stage.
Diagnostics

Timely diagnosis of heart failure is one of the most effective treatment mechanisms, allowing timely prescribing of conservative therapy.
In addition to differential analysis of anamnesis and objective vital signs, full complex laboratory and instrumental examinations - chest x-ray, echocardiogram, etc.
Most patients admitted to the hospital with a diagnosis of heart failure require complex treatment, often with surgery.
Medication

- Prescription of beta blockers, which reduce heart rate and blood pressure. This prevents overload of the heart muscle.
- Combating the symptoms of heart failure with the help of glycosides (digoxin, corglycon).
- Using diuretics to remove excess fluids from the body.
Unfortunately, in most cases conservative therapy not enough to overcome the disease, especially in the severe stage of heart failure. In this case, it is rational to use surgical intervention - replacing valves, unblocking arteries, installing a defibrillator or pacemaker.
Additional recommendations for patients include following a diet with a minimum of salt and liquid, normalizing overweight, physiological procedures, proper cardio exercises, taking specialized vitamin complexes, as well as quitting smoking/alcohol abuse.
Alternative
A number of alternative modern studies show that in the complex treatment of heart failure, individual dietary supplements and compounds (coenzyme Q10, taurine) contribute to more effective treatment of the disease and speedy recovery. This is due to the peculiarities of the pathogenesis of chronic forms of heart failure and the destruction of macroenergetic compounds at the cellular level, which leads to the activation of free-radial reactions and the formation of biophysical processes that catalyze the development of the disease.
Thus, regular intake of flavonoids and taurine in a number of patients improves the endothelial function of patients with heart failure by inhibiting platelet function. However, the use of the above-mentioned drugs is possible only after preliminary consultation with the attending physician and only in combination with standard conservative therapy.
Treatment with folk remedies

Traditional medicine can offer the patient a huge number of different recipes for the prevention and treatment of heart failure as a supplement complex therapy diseases. Any folk remedies can be used only after prior agreement with your cardiologist!
- Pour a liter of water over half a kilo of fresh hawthorn fruits and boil for twenty minutes, then strain, adding 2/3 cup of honey and sugar to the broth. Mix thoroughly, cool and consume two tablespoons. spoons before each meal for one month.
- Take a tablespoon of fresh viburnum, mash it until the juice appears and pour a glass of boiling water, adding two teaspoons of honey. Let the decoction brew for one hour, then take ½ cup twice a day for 1 month.
- 10 milliliters alcohol tinctures digitalis, lily of the valley and arnica, mix with 20 milliliters of hawthorn tincture and take three times a day (30 drops at a time) for four weeks.
- Pour two tablespoons of crushed dried adonis with a glass of boiling water, transfer to a thermos and let it brew for two hours. Strain the tincture and drink 50 milliliters of liquid three times a day for two weeks.
Consequences of heart failure
Complications and consequences of HF are nonspecific and depend on the stage of the disease. The most common:
- Heart rhythm disturbances and death. People with heart failure die 44 percent more often than people without heart failure.
- Bronchopneumonia and infectious lesions. Due to stagnation/transudation of fluids and blood, as well as low respiratory activity, very favorable conditions arise for the development of infections respiratory tract and lungs.
- Pulmonary hemorrhages. The symptom that accompanies HF with pulmonary edema and cardiac asthma is one of the earliest complications of the disease.
- Liver cell failure. Changes in liver function due to venous stagnation and deterioration of perfusion.
- Cardiac cachexia. It is a complication in the terminal stages of heart failure and is caused by metabolic disorders, in particular poor absorption of fats, leading to generalized anorexia.
- Embolisms, infarctions of the lungs and other internal organs due to blood stasis.
- Chronic renal/cardiocerebral failure, decompensation of the function of the digestive canal system without arterial occlusion - a complication caused by low MOS.

Diet - important element complex treatment, rehabilitation and prevention of a person before, during and after heart failure. The general principles of proper nutrition during this period are aimed at correcting the daily intake of salt and liquids. The food should be easily digestible and fairly high in calories.
The optimal nutrition plan is fractional, divided into 5–6 approaches. Be sure to exclude strong varieties of tea and coffee, chocolate, fatty, smoked, salty foods, and pickles from your diet. If the patient’s condition is satisfactory, then during the remission stage the maximum amount of salt consumed per day should not exceed 5 grams. In case of destabilization and exacerbations or acute form of heart failure, food containing salt should be completely excluded from the diet.
Also, check daily use liquids in the range of 0.8–1.5 liters per day (this includes both water and liquid soups/borscht, teas, juices, and other products). Increase your intake of foods containing potassium - nuts, raisins, bananas, baked potatoes, veal, peaches, Brussels sprouts, buckwheat and oatmeal. This is especially true if you are prescribed diuretics to remove excess fluid from the body and reduce swelling.
Useful video
Heart failure. What makes the heart weak?
Heart pain, what to do, how to help and prevent - Doctor Komarovsky
 Cardiomyopathy is one of the causes of acute left ventricular heart failure
Cardiomyopathy is one of the causes of acute left ventricular heart failure 
 Symptoms of left ventricular failure
Symptoms of left ventricular failure 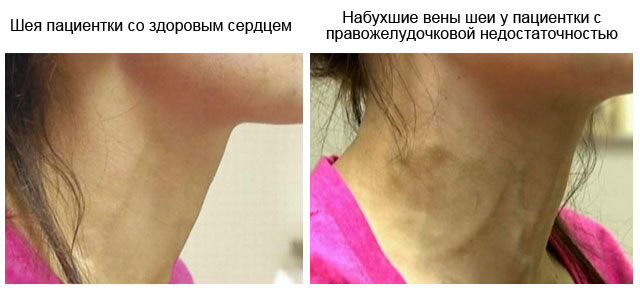
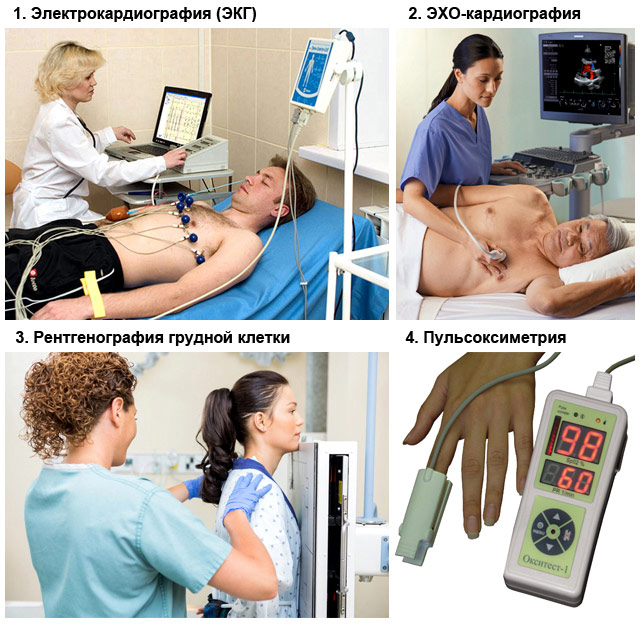 Methods for diagnosing acute heart failure
Methods for diagnosing acute heart failure