Dream interpretation of a dead man being alive
Dream interpretation is an ancient art that allows you to at least assess the psychological status of a person, because...
Ultrasound examination helps diagnose certain pathologies associated with an unfavorable pregnancy. Already during the very first routine ultrasound it is possible to identify Not full presentation chorion
Many women would like to know why incomplete chorion presentation occurs, what it is and why it is dangerous. Only narrow specialists can answer this question. The chorion is the outer shell of the embryo. It is covered with numerous villi. Over time, the chorion turns into the placenta. On early stages During pregnancy, it is the villous membrane that transports nutrients to the embryo, protects the embryo, and also performs excretory and respiratory functions.
If pregnancy proceeds without pathologies, the chorion develops in the area of the uterine fundus. Usually this is exactly what happens, with the placenta subsequently attaching predominantly to the back or front wall. When presenting, the chorion is located in the lower part of the uterus. The internal pharynx is partially blocked.
There are many reasons why this pathology develops. These include:
Availability inflammatory diseases genital area;
Uterine fibroids;
Irregular structure of the uterus;
A large number of births in the anamnesis.
How dangerous is partial presentation? Doctors consider this a rather serious pathology, but it all depends on how severe it is. In this situation, the chorion covers only the area of the internal os of the uterus. With marginal presentation, there is a chance that in the future the placenta will begin to form a little higher and the pregnancy will proceed without complications.
Central incomplete chorionic presentation usually leads to complete placenta previa. This pathology serves as an indication for cesarean section. When the internal uterine os is blocked, natural childbirth is simply impossible.
Incomplete chorion presentation not only leads to improper formation placenta. A woman may encounter a number of complications not only during childbirth, but also during pregnancy. different stages pregnancy. The most common and very dangerous complications include:
Termination of pregnancy is spontaneous;
Hypoxia;
Intrauterine fetal death;
Bleeding;
Often, it is during partial presentation that a woman notices a scarlet discharge from the genital tract. Sexual intercourse or taking a hot bath can provoke the development of bleeding.
Install this diagnosis is possible only after the woman has undergone an ultrasound diagnosis. Unfortunately, this pathology not treated. It is simply impossible to move the chorion to another part of the uterus. After diagnosing incomplete presentation, all efforts of doctors and the patient herself should be aimed at maintaining the pregnancy. If pain or bleeding occurs, gynecologists usually offer the expectant mother hospital treatment. It is very important in such a situation to strictly observe bed rest and be under medical supervision around the clock. Iron supplements may be prescribed to prevent anemia. In case of incomplete chorion presentation, sexual intercourse is strictly prohibited, as well as performing heavy loads, heavy lifting and overwork. This can lead to very sad consequences.
If a woman has already had pregnancies with incomplete chorionic presentation, the risk of pathology occurring with repeat pregnancies rises. Unfortunately, it is very difficult to prevent such developments, but it is possible with a competent approach to conception planning.
Incomplete chorion presentation is quite serious and dangerous pathology. It is very important to diagnose it on time and take all measures aimed at preserving such a pregnancy. The best results can be achieved with inpatient treatment.
In order to understand why a low position of the chorion is dangerous, let’s define what a presentation is. So, chorion presentation is a pathology of pregnancy in which it is located in the lower part of the uterus. In this case, the chorion partially or completely covers the internal os.
The reasons for chorionic villus presentation are not clear, but some factors are known that influence chorionic villus presentation: uterine fibroids, uterine developmental abnormalities, postoperative scars on the uterus, chronic inflammation uterus, chorionic presentation in previous pregnancies, frequent abortions. Chorionic presentation along the anterior wall or presentation can also occur due to polyps or multiple fibroids. That's why frequent visit gynecologist for preventive examinations and healthy image life will help to avoid problems associated with possible presentation and its consequences during pregnancy.
This classification of chorion presentation is accepted. Complete chorion presentation is dangerous due to the complete occlusion of the internal os of the cervix. It is also called central chorionic presentation. This arrangement is dangerous due to severe bleeding due to placental abruption, and hypoxia is dangerous for the child at this time, due to which he can die in a matter of minutes.
Partial chorion presentation means that only part of the internal os is blocked. Low chorion presentation means that the chorion does not cover the internal os, but is located at a distance of less than 3 cm from it.
During pregnancy, the placenta migrates all the time, so even complete placenta previa may become normal before delivery. Chorionic presentation is an indication for caesarean section; natural childbirth is excluded in this case.
There is no cure for breech presentation as such, the main thing is to stick to it. preventive measures. The best prevention- a healthy lifestyle and regular visits to the doctor, identifying and monitoring the appearance of fibroids and polyps before pregnancy. If, however, chorionic villi previa was detected during pregnancy, it is necessary to stop sexual relations, reduce physical activity to a minimum, and exclude stressful situations and limit mental stress, take a complex and medications to reduce the tone of the uterus, as well as iron supplements to prevent anemia.
Regular ultrasound examinations will help to qualitatively control the current situation, and maybe in the third trimester the placenta will migrate safely and become established in safe place which will lead to natural childbirth.
Contents:
| Maturity level | Weeks of pregnancy |
| Zero (0) degree | 20-30 |
| First (1) degree | 30-34 |
| Second (2) degree | 34-37 |
| Third (3) degree | 37-39 |
Determining the degree of placental maturation is necessary in order to understand whether the placenta is capable of supplying a sufficient amount of nutrients to the developing baby.
As pregnancy progresses, the thickness of the placenta increases. This is a normal process. The thickness of the placenta is determined using ultrasound (see. Ultrasound during pregnancy).
The normal thickness of the placenta is different dates pregnancy is presented in the table below.
| Gestational age | Normal thickness placenta in millimeters |
| Week 20 | 16,7-28,6 |
| 21 weeks | 17,4-29,7 |
| Week 22 | 18,1-30,7 |
| Week 23 | 18,8-31,8 |
| Week 24 | 19,6-32,9 |
| Week 25 | 20,3-34,0 |
| Week 26 | 21,0-35,1 |
| Week 27 | 21,7-36,2 |
| Week 28 | 22,4-37,3 |
| Week 29 | 23,2-38,4 |
| Week 30 | 23,9-39,5 |
| 31 weeks | 24,6-40,6 |
| Week 32 | 25,3-41,6 |
| Week 33 | 26,0-42,7 |
| 34 week | 26,8-43,8 |
| Week 35 | 27,5-44,9 |
| Week 36 | 28,2-46,0 |
| Week 37 | 27,8-45,8 |
| Week 38 | 27,5-45,5 |
| Week 39 | 27,1-45,3 |
| Week 40 | 26,7-45,0 |
Like the degree of maturity, the thickness of the placenta is important for assessing how adequately the placenta supports the development of the child.
This paragraph was added after receiving the question:
Aging of the placenta is said to occur in cases where calcifications appear in the tissues of the placenta (deposition of calcium salts in areas that have “already exhausted their resource” and do not function). Calcifications are clearly visible on ultrasound, and it is this examination that is used primarily to determine the degree of maturity of the placenta.
To a certain extent, the gradual “switching off” of placental tissues and the deposition of calcifications in them is a normal process (normal, physiological maturation placenta). It is believed that the placenta should reach its maximum degree of maturity (grade 3) at 37-40 weeks.
ABOUT premature ripening(aging) of the placenta is said in cases where multiple calcifications (3rd degree of maturity) appear in the placenta in women who have not yet reached 37 weeks. Usually, women learn about the premature maturation of their placenta after the next ultrasound performed after the 30th week of pregnancy.
Quite often the reasons premature aging placentas remain unknown. However, it is known that the development of this disorder can be facilitated by arterial hypertension , gestational diabetes and smoking.
Despite the fact that signs of premature aging of the placenta are rarely detected in women who have not yet reached 40 weeks of pregnancy, the detection of multiple calcifications in the placenta (3rd degree of maturity) does not always mean a threat to the development of pregnancy or the health of the pregnant woman. One study conducted in 2011 showed that the likelihood of developing complications largely depends on the stage of pregnancy at which premature aging of the placenta was detected.
As part of this study, the development of pregnancy in women from three groups was monitored:
The results of the study showed that in women in group 1, complications such as premature birth, low birth weight, premature placental abruption, bleeding after childbirth, and stillbirth were observed much more often than in women in group 3. At the same time, among women from group 2, the risk of developing any problems during or after childbirth was the same as in group 3.
The results of this study suggest that the appearance of calcifications (grade 3 placental maturity) before 32 weeks of pregnancy does increase the risk of various complications, while the identification of signs of premature aging of the placenta after 32 weeks means that there is no serious reason to expect any complications that may be related to this.
Currently, to assess the condition of the fetus in late pregnancy, doctors often prescribe Doppler ultrasound, with which the doctor can assess the condition of the placental vessels and the rhythm of the fetal heart and, accordingly, the degree of supply of oxygen and nutrients to the fetus.
In terms of assessing the ability of the placenta to support fetal development, Doppler ultrasound gives more information than conventional ultrasound, which can only assess the structure of the placenta. Many experts believe that if Doppler ultrasound readings are normal, the presence of calcifications in the placenta should not be a cause for concern.
What should I do if I have premature aging of the placenta?
As mentioned above, if signs of premature aging of the placenta appear before 32 weeks, fetal development may be disrupted and the risk of other complications may increase. In this regard, if you have discovered signs of premature aging of the placenta, the doctor may prescribe you a series of repeated ultrasounds during which the rate of fetal development and its development will be checked. general state. If doctors notice signs that the fetus is actually receiving less oxygen or nutrients than it needs, they may recommend a cesarean section or induction of labor.
Immediately after the birth of the child, the placenta (baby place) begins to quickly peel off from the wall of the uterus and approximately 15-30 minutes after birth it is completely removed from the uterine cavity. This process is called “birth of the placenta.” Due to the fact that the size of the placenta is significantly smaller sizes newborn baby, the birth of the placenta in most cases occurs easily and painlessly.
Immediately after the birth of the placenta, the gynecologist carefully examines it to determine whether part of the placenta remains in the uterine cavity. Preservation of even small fragments of the placenta in the uterus can cause severe postpartum bleeding, and in the future can cause infection and even malignant tumor(see Chorionepithelioma).
The development of pregnancy begins with the attachment of a fertilized egg to one of the walls of the uterus (see also how does conception occur?). As already mentioned at the beginning of the article, in the first stages of pregnancy, the fetus is attached to the wall of the uterus with the help of the chorion; at the end of the 1st trimester of pregnancy, the placenta forms in place of the chorion.
The uterine cavity can be schematically described as a cube. The developing embryo can attach to the upper, posterior, one of the lateral (right or left) or lower walls of the uterus.
Chorionic previa (placenta) is an incorrect location of the placenta when, instead of the body of the uterus, it captures partially or completely the lower uterine segment. Chorion is synonymous with placenta in the early stages of development. By the end of pregnancy, in most patients the chorion rises, but there are exceptions. If the localization of the chorion is posterior, then it will rise more slowly, if it is anterior, then faster.
Causes of the disease
Accurate and credible reasons The occurrence of this disease is unknown, but there are a number of factors that contribute to the development of this disease. In particular, chorionic presentation can develop due to:
In addition, we can say that chorionic presentation is quite common in early stages pregnancy, statistically this is up to 30% of cases.
Symptoms of the disease
The main symptom of the disease is the appearance of bleeding, which appears due to the fact that the placenta is not capable of stretching, so when the uterus stretches, it peels off and causes bleeding. Bleeding can appear spontaneously, then disappearing, then appearing again, while the pain disappears. The low location of the chorion contributes to heavy bleeding. In addition, bleeding can be triggered by factors such as physical activity, vaginal examination, sexual intercourse, hot bath, sauna, and also constipation.
Complications that can cause chorionic presentation
The main complication that this disease gives is unplanned termination of pregnancy or premature birth. With this disease, the child develops normally, but patients experience characteristic hypotension, so even slight blood loss leads to anemia. If the bleeding began spontaneously, then sometimes it is necessary to take the last measure in order to save the life of the mother and baby.
Diagnosis of the disease
Diagnosis of presentation usually does not cause difficulties in a patient who is normally observed in the hospital. This disease can be easily diagnosed with a routine ultrasound examination. It is not recommended for pregnant women.
If the patient has not undergone an ultrasound examination, then this disease can be recognized by the fact that it is not accompanied by painful sensations, as well as by the high position of the uterine fundus.
Treatment of the disease
First of all, it must be said that all medications for this pathology are absolutely useless, because they cannot in any way affect the location of the chorion. If suspicious symptoms appear and the disease is diagnosed, it is necessary to completely exclude any physical activity, as well as completely avoid sexual contact. In addition, the patient needs constant supervision by a specialist, so she is hospitalized in the hospital.
In the event that there is no constant bleeding, the patient may well stay at home, while resting more often and eating properly, choosing a diet to prevent constipation. It should be noted that this is especially important, because with this pathology any laxatives are contraindicated.
If the patient has a complete chorionic presentation, then natural childbirth is contraindicated for her and is required. Natural childbirth is at great risk, resulting in large blood loss, which will threaten the health of both mother and child.
The first weeks of pregnancy for the expectant mother are probably one of the most difficult periods throughout the entire period of bearing a child. At this time there are several “ critical periods"in the life of the future little man, his mother is mentally and physically rebuilt for successful pregnancy. Unfortunately, this period does not always pass without complications and problems, so routine ultrasound examinations should be carried out. A woman’s first ultrasound is scheduled for the end of the first trimester, and it is at this time that this pathology is most often detected.
How dangerous is chorionic presentation at 12 weeks, and how to prevent complications?
The chorion is a special organ that provides communication between the body of the mother and her unborn child. In fact, this is an early stage of the development of the placenta, therefore the term “chorion” is used only during the first three months of gestation, after which the word “placenta” is already used. One surface of the chorion faces the fetus, and the other is attached to the wall of the uterus. And it is precisely when the location of the chorion is atypical that various disorders can occur.
As you know, the uterus communicates with the vagina and external genitalia through the cervix, inside which there is a special cervical canal. The internal opening of this canal, which opens into the uterus, is called the os cervical canal. The chorion or placenta is normally attached to the bottom or lateral surfaces of the uterus and does not overlap the pharynx in any way. But in some cases they can partially or completely close the internal opening of the cervical canal - it is in this situation that a disorder called "Chorion presentation"
The closure of the cervical canal by the chorion does not have to be complete, therefore there are several types of presentation that characterize the complexity of this condition:
Partial chorion presentation. In such a situation, the developing placenta covers at least two-thirds of the lumen of the cervical canal.
Regional presentation chorion . This is a variation and, one might say, an easier version of partial presentation, since only one third of the lumen of the pharynx is covered.
Central chorion presentation. In this case, the lumen of the pharynx of the cervical canal is completely closed by the future placenta, which significantly complicates the course of pregnancy and poses a threat to both the unborn child and the life of the mother.
Low location of the chorion . The forming placenta can be located next to the opening of the cervix, but does not block it. If it is attached near the edge of the pharynx closer than three centimeters, then it is said to be low. This is not dangerous, but poses a potential threat to pregnancy.
Chorionic presentation at week 12 can be in any of these forms.
As pregnancy progresses, the growing uterus can pull back the placenta, so central presentation can turn into partial and marginal, and then disappear completely. According to obstetricians, more than 90% of cases of one or another chorionic presentation completely disappear over time, so if you were diagnosed with it in the first weeks of pregnancy, this is not a reason to panic. But you will have to monitor your condition and not neglect examinations by a specialist.
Why exactly the developing placenta is attached in such dangerous proximity to the pharynx of the cervical canal is completely unknown. However, several main factors have been noted that contribute to more likely development of this complication during pregnancy. Especially often various options Chorionic presentation develops in women who have had in the past or currently have the following diseases and conditions:
Inflammatory lesions uterus, abortion, especially using the curettage method, surgical interventions for fibroids or cesarean section. All these factors are united by one consequence - after this, inner surface The uterus may leave scars and adhesions, which make it difficult for the chorion to attach to the “right” place.
Diseases of the liver, kidneys or heart. It would seem, how can these conditions affect the position of the fetus and its placenta in the uterus? But with pathologies of these organs, blood stagnation may occur in the pelvic area, which contributes to lower attachment of the chorion.
Multiple births in the past. If you are pregnant not for the first time, then your chances of improper attachment of the chorion significantly increase. Most physiologists see the reasons for this phenomenon in the fact that after each pregnancy, in the area of the uterus where the placenta was attached, the structure of the endometrium changes. Therefore, at the next conception, the chorion can no longer attach there. Over time, such places on the inner surface of the uterus become less and less, which leads to the attachment of the placenta in the danger zone.
Uterine deformities, acquired (for example, after surgical interventions) or innate nature, can also lead to chorionic presentation.
Most pregnant women are frightened by such a conclusion from the first ultrasound examination. Although in fact, chorionic presentation during pregnancy of 10-13 weeks is observed in approximately 5% of cases, that is, in every twentieth woman. In more later this condition is becoming increasingly rare, occurring before birth in no more than 0.5% of women in labor. main reason This lies in the fact that the growing uterus is able to “pull” the point of attachment of the chorion from the pharynx of the cervical canal to a more safe zone. Therefore, according to pediatricians, chorion presentation during the first trimester can be regarded as a feature of the course of pregnancy, but not a complication.
Difficulties begin if the presentation continues to persist after the third month of pregnancy. Being dangerously close to the pharynx of the cervical canal, the placenta can be easily injured, which leads to bleeding varying degrees expressiveness. With marginal or partial presentation, the first spotting occurs closer to the sixth month. They are practically painless, and blood may be released in thin streaks in the discharge, or give the impression of menstruation. Central presentation can manifest itself with such symptoms as early as the second or third month. In fact, this is the main consequence and danger of chorion presentation, which entails whole line disturbances in the course of pregnancy and the health of the mother and her unborn child:
The constant loss of small amounts of blood leads to anemia in a pregnant woman. You may experience weakness, dizziness, skin become pale. When heavy bleeding may decline arterial pressure, your vision becomes dark, you can even lose consciousness.
Disruption of connections between the uterus and placenta also leads to malnutrition of the unborn baby. Its development slows down, and against the background of reduced oxygen delivery (due to a damaged placenta and anemia in the mother), intrauterine fetal hypoxia occurs.
If the mother’s blood loss reaches significant levels, this can lead to miscarriage, intrauterine fetal death and a number of other terrible consequences.
In addition to the problems described, presentation is often complicated by incorrect positioning of the fetus, which leads to difficulties during the birth process. Therefore, if such a condition is diagnosed in you in the sixth month or later, then you need to mentally prepare yourself for what you may have to do C-section rather than giving birth on your own.
Unfortunately, at the moment, doctors do not yet know how to correct such a condition as chorionic presentation, so all treatment comes down to preventing complications and eliminating their consequences. As a rule, if there is a central presentation in the fourth month, they prefer to place the girl in the position in a hospital for preservation. The same is done with partial forms of presentation, if they are complicated by bleeding, hypertonicity of the uterus and other factors that may threaten termination of pregnancy. In a hospital setting you will be provided with the following treatment:
To begin with, strict bed rest and restriction physical activity, which is one of the most important factors prevention of bleeding with placenta previa. In addition, you will need to avoid emotional stress, as this can also lead to negative consequences.
Regular examination by a doctor and diagnostic tests ultrasound examinations. Being under 24-hour medical supervision, you greatly reduce the risk of sudden complications, since they will be identified and corrected as soon as possible. Most deplorable and even tragic situations with chorion presentation are caused by delayed medical intervention.
Maintenance treatment, which includes all the vitamins necessary for the pregnant body.
Proper and regular nutrition, which helps normalize work gastrointestinal tract. If you have diarrhea or constipation, you may strain your abdominal muscles, which increases pelvic pressure and may become trigger factor bleeding.
If you develop anemia due to bleeding, it can be treated in a hospital setting by taking iron supplements, including those given by injection.
Treatment is also prescribed to eliminate other factors that threaten the course of pregnancy - for example, antispasmodics for uterine hypertonicity.
With partial chorion presentation, which does not manifest itself severe symptoms, you don’t have to go to bed for conservation, but you need to take certain precautions to prevent possible complications. These primarily include:
Exercise stress. Leisurely walks and walking around the house is the maximum for a girl in such a situation. Lifting heavy objects, walking up stairs, and running are strictly contraindicated.
It is necessary to completely avoid sexual contact. During pregnancy, in principle, sexual intercourse is not prohibited at almost any stage, but during presentation it can cause severe bleeding.
Mental stress or stress affects the pregnant body no better than lifting weights. Therefore, they also need to be excluded, and even with sedentary and predominantly mental work, it will be time for you to go on maternity leave.
Also, as with preservation, it is necessary to eat properly so as not to cause changes in stool and at the same time provide the body with all the necessary nutrients. You also need to agree on the choice with your doctor. vitamin complex, which will be very useful in such a situation.
And most importantly, if you have been diagnosed with chorion previa and at some point you notice the release of even a small amount of blood in the absence of pain, weakness and other symptoms, then you need to urgently consult a doctor. And if the bleeding is accompanied by pain in the lower back and lower abdomen, palpitations, weakness or fainting, then you need to call an ambulance as soon as possible, as you risk losing your child.
"- similar diagnosis can be found in medical card pregnant quite often. In the first half of pregnancy, the “embryo” and “chorion” are medical terms, personifying the child and the placenta, respectively. Chorionic presentation indicates the site of attachment of the future placenta to the uterine wall, which may suggest further development fetus in the uterine cavity. In order to accurately consider the issue, such medical terms should be analyzed in detail.
The chorion is a continuation of the umbilical vein of the embryo. It attaches to the wall of the uterus, as a result of which the embryo, and later the child, will receive all the necessary and beneficial nutrients that directly affect the development of the fetus.
The chorion attachment is formed in three places:
Normal attachment of the chorion is its attachment to the bottom or sides of the uterus. In 10-12% of cases, the chorion is attached to the cervix. This position is called presentation. Depending on the location of attachment, there are also several varieties of the presented diagnosis.
At the end of the first semester, the pregnant woman is assigned the first. Here you can find a similar diagnosis of the attachment of the future placenta. It is necessary to consider the presented medical terms in more detail.
It should be noted that chorion presentation at 12 weeks does not mean its permanent location until birth. Very often a kind of migration occurs. Similar processes are carried out until week 20. Sometimes you can observe migration at quite a late stage - almost before birth.
Chorionic presentation at 13 weeks indicates the place of attachment in the cervical cavity. Such features of the development of pregnancy have practically no effect on the development of the fetus, however, one should not deviate from general rules maintaining pregnancy. Typically, chorionic presentation at 13 weeks prohibits sexual intercourse for pregnant women, as well as any heavy lifting. You should not expose yourself to stress and physical activity.
Otherwise, the woman faces heavy bleeding during detachment. placental tissue. Therefore, a woman should take care of herself and her child, because heavy bleeding can provoke hemorrhagic shock, from which the expectant mother can die. Even the slightest bleeding threatens the child with the loss of the required amount of oxygen and nutritional components.
As already described above, chorion presentation has several varieties. They, in turn, influence the further development of the fetus, as well as the result of the form of delivery - natural or cesarean section. Regional presentation of the chorion at 12 weeks is the most favorable outcome that can develop with the presented pathology. This type of pathology can “eliminate on its own” as a result of migration within a few days or weeks.
Regional presentation of the chorion is characterized by partial overlap of the cervix. The presented species is divided into two subspecies. Thus, they distinguish between marginal presentation of the chorion at the 13th week, where the future placenta covers no more than 1/3 of the cervix, and incomplete attachment, which entails more dangers and difficulties, since this diagnosis is made in the case of overlap of 2/3 of the cervix. Both subspecies have the ability to migrate, so the expectant mother should not worry. Most women give birth on their own, even if they were once diagnosed with marginal chorionic presentation at 12 or 13 weeks.

Low chorion presentation occurs in only 5% of cases. This pathology is explained by the attachment of the future placenta 2-3 cm below the cervix. These features are diagnosed in pregnant women in the first two trimesters, so there is no need to talk about any surgical interventions, because by birth the placenta takes its normal position through migration.
Central chorionic presentation is the reason for the majority of deliveries performed by cesarean section. Most often, a pregnant woman in this case, already from the 4th month of pregnancy, is admitted to a hospital for full examination and appropriate observation, since complete occlusion of the cervical canal of the cervix may lead to unexpected uterine bleeding.
It turns out that the diagnosis of “marginal chorionic presentation” should not entail serious problems and provoke serious nervous condition pregnant woman. If there are designations and diagnostics that are unclear to you, you should check with your doctor what this or that term means.
Home " Problems " Echographic signs of a low location of the chorion. Chorionic presentation - causes, symptoms, treatment
Chorion, or villous membrane- This outer shell embryo, covered with numerous villi that grow into the inner lining of the uterus.
The chorion begins to function in the early stages of pregnancy and performs a number of functions:
On initial stages During development, the villi do not contain vessels; only by the end of the first month the process of their formation (vascularization) begins, and blood circulation develops, which ensures an intensive exchange of nutrients and oxygen between the mother’s body and the embryo.
Initially, the villi evenly cover the entire surface of the chorion; from the second month, their gradual atrophy begins on the side facing the uterus and intensive growth on the fetal part.
The final transformation of the chorion into the placenta occurs towards the end of the third month - the beginning of the fourth month of pregnancy.
At normal course During pregnancy, the chorion develops in the fundus of the uterus, moving to the anterior, posterior and lateral walls.
Information Chorionic presentation- This pathological condition, in which the chorion is located in the lower part of the uterus and partially or completely covers the internal os of the cervix.
The reasons for the incorrect location of the chorion have not been fully elucidated, but several factors that may contribute to the development of this pathological condition:
The following types of chorion presentation are distinguished::
Regional presentation- this is the most favorable form: the risk of complications is minimal; in most cases, as the uterus grows, the chorion migrates upward and takes the correct position.
Most dangerous looking is complete chorion presentation.
In most cases, chorionic previa is diagnosed by performing an ultrasound examination with complete absence complaints from the woman. Less commonly, an incorrectly located chorion manifests itself by the appearance of varying degrees of intensity (from spotting to heavy bleeding) against the background of complete health. As a rule, the occurrence uterine bleeding contribute external factors(physical activity, sexual intercourse, etc.).
Chorion and placenta previa are one of the most serious pathologies in obstetrics, because may cause to a number of complications, both from the fetus and from the mother:
It should be noted that specific treatment this pathology is absent: artificially it is impossible to change the location of the chorion, therefore all therapeutic measures are aimed only at maintaining pregnancy and treatment possible complications.
However, diagnosing chorionic presentation does not mean that in the future the formed placenta will also occupy an incorrect position. Due to the growth of the uterus, upward migration of the chorion and placenta is possible.
Tactics for further management of pregnancy when chorion previa is detected, it depends on the presence of bleeding and its volume.
If chorionic presentation is diagnosed by ultrasound and there is no bleeding, it is advisable to hospitalize the woman in a hospital, where a set of therapeutic measures is carried out:
When bleeding occurs carry out similar treatment ( mandatory in a hospital setting!), but in addition, hemostatic drugs (sodium ethamsylate) are prescribed. In most cases, therapeutic measures are effective, and pregnancy can be maintained further.
Important For massive bleeding the development of conditions that threaten the woman’s life is possible; in this case, regardless of the gestational age, the pregnancy is urgently terminated.
According to statistics, up to 45% of pregnant women face such a diagnosis as marginal chorionic presentation in the early stages of pregnancy. Should you be afraid of such a medical verdict, and what to do, will be discussed in this article.

The chorion is a temporary organ that performs the functions of a pharmacist. It is formed from the moment of implantation of the fertilized egg from fallopian tube, where the meeting of the egg and sperm took place, into the uterine cavity. As soon as the blastocyst (which is what the fertilized egg turns into by 8-9 days after ovulation) reaches the uterine cavity, it strives to gain a foothold in it. It is this process that is called implantation.
At the site of attachment of the blastocyst shell, special enzymes are secreted that make the mucous membranes of the uterus more pliable and allow the fertilized egg to “grow.” A chorion is formed at the site of attachment. It is necessary to supply the fertilized egg with useful substances from the mother’s blood. A little later, the placenta appears in its place. But until the 12-13th week we are talking specifically about the chorion, since the placenta is still forming and does not function.

If implantation is successful, the fertilized egg is fixed in the fundus of the uterus (this is its top part). If for some reason pathological reasons The blastocyst failed to implant in the upper or middle part of the uterus; it may descend into the lower uterine segment. And then the chorion will form low.
Chorionic presentation is its location relative to the cervical canal - a thin passage inside the cervix connecting the uterine cavity and vagina. There is no talk of presentation only if the chorion has formed in the area of the fundus of the uterus or in its middle part (in the body of the uterus).


If the chorion is low, there are several types of presentation.
Depending on the degree of occlusion of the cervical canal, through which the fetus will then pass during childbirth, There are also types of pathology.

Any chorion presentation, but especially complete and incomplete, poses a threat of miscarriage and chorion detachment. In its place, the placenta will form, a network will develop blood vessels, and this is dangerous if the vessels grow into the lower part of the uterus, which, according to the laws of nature, should open and release the baby out when the due date comes.
Often, chorion previa can develop into another pathological condition - placenta previa, and then spontaneous childbirth naturally, most likely, will be contraindicated. The woman will have a caesarean section. Carry the child to due date It will also not be easy, since the low-lying placenta and adjacent to the exit from the uterus will create a risk of spontaneous bleeding at any time.
A baby who is breech will receive less oxygen and useful substances, and this is fraught with malnutrition and hypoxia.

The main reason for marginal presentation is internal conditions that prevented the fertilized egg from implanting normally and in a more suitable fundus of the uterus. Such prerequisites include disorders of the endometrium of the uterus. It is usually observed in women who have had several abortions or have undergone diagnostic curettage.
Miscarriages and a history of frozen pregnancies also increase the likelihood of abnormal placement of the fertilized egg. An obstacle to full implantation may be a scar or several scars on the uterus from previous operations or a cesarean section.
Women who have given birth a lot cannot boast of being strong and elastic. muscle tissue reproductive organ, they also have an increased likelihood that a subsequent pregnancy may occur against the background of low placentation.

The presence of fibroids, fibroids and other formations in the upper part of the uterus also creates obstacles for the attachment of the blastocyst, and it is forced to descend in search of “shelter” in the lower uterine segment. The reason may also be congenital anomaly structure of the uterus - bicornuate or saddle uterus. A certain sequence of such pathologies has also been noticed - if in a previous pregnancy a woman had low placentation, it is highly likely that the attachment of the fetus and the development of the chorion during a subsequent pregnancy will also be low.
There may be no symptoms of marginal chorionic presentation in the early stages, but small short-term symptoms may appear. bloody issues. Usually they are always assessed correctly by a woman - as a threat to the preservation of the child.
If the chorion, and subsequently the placenta, does not migrate, such bleeding, associated with the rupture of small blood vessels due to stretching of the uterine walls, can recur frequently, in some cases until the very birth. Because of them, a woman begins to suffer from anemia, she chronically lacks iron, and her blood contains a small amount of hemoglobin. Be that as it may, if bloody discharge appears from the genital tract of a pregnant woman, you should immediately call an ambulance.
With timely hospitalization using conservative treatment It is possible to save up to 90% of all babies who grow in the mother's womb against the background of marginal presentation of the chorion, placenta and even the umbilical cord.

As already mentioned, marginal chorionic presentation is diagnosed in approximately 4-5 women out of ten pregnant women up to 12 weeks. However, not all of them immediately fall into the risk group and are listed as patients for planned cesarean section. The prognosis is favorable, and in 90% of cases the chorion, and then the placenta, which forms in its place, migrates higher along with the growth of the uterus.
The baby in the mother's womb is growing rapidly. To meet his needs for comfort, the walls of the uterus and the ligamentous apparatus are forced to stretch. Together with them, the placenta, which at the beginning of pregnancy was in a marginal presentation, will “crawl” upward. On the front or back wall the uterus will the placenta migrate - it doesn’t matter. It is important that in most cases it actually rises, and all the threats and risks associated with low placentation remain a thing of the past.

Medicine cannot influence the migration process, speed it up or stimulate it. A woman diagnosed with marginal chorionic presentation must follow all the recommendations of her attending physician, exclude physical activity, heavy lifting, jumping, sudden movements, squats. She will have to visit her doctor more often and have an ultrasound done to monitor the process of chorion (placenta) migration. Sex during marginal presentation is prohibited, since orgasm associated with contraction of the muscles of the uterus can contribute to rapid traumatic detachment of the chorion and the occurrence of severe bleeding, in which the child can die in utero, and the woman can lose a lot of blood and die from this.
The process of placental migration is usually completed by 18-20 weeks of pregnancy. By this time or a little later (by 35-28 weeks), the true state of affairs becomes clear - if the placenta has risen, the restrictions will be lifted, if not, the pregnant woman will be classified as a risk group for premature birth and will continue to lead with increased attention and awe.

It is impossible to speed up migration, but treatment for a woman with marginal chorionic presentation will most likely be prescribed. Only it will not be aimed at the chorion itself, but at relaxing the muscles of the uterus, so as to prevent its tone and not provoke new detachments and bleeding. Depending on the degree of presentation, treatment may be carried out in a hospital, or they may be allowed to take necessary medications at home. The doctor leaves this question at his own discretion.
The first weeks of pregnancy for expectant mother are probably one of the most difficult periods throughout the entire period of bearing a child. At this time there are several “critical periods” in the life of the future little man; his mother is mentally and physically rebuilt for a successful pregnancy. Unfortunately, this period does not always pass without complications and problems, so routine ultrasound examinations should be carried out. A woman’s first ultrasound is scheduled for the end of the first trimester, and it is at this time that this pathology is most often detected.
How dangerous is chorionic presentation at 12 weeks, and how to prevent complications?
The chorion is a special organ that provides communication between the body of the mother and her unborn child. In fact, this is an early stage of the development of the placenta, therefore the term “chorion” is used only during the first three months of gestation, after which the word “placenta” is already used. One surface of the chorion faces the fetus, and the other is attached to the wall of the uterus. And it is precisely when the location of the chorion is atypical that various disorders can occur.
As you know, the uterus communicates with the vagina and external genitalia through the cervix, inside which there is a special cervical canal. The internal opening of this canal, which breaks off into the uterus, is called the os of the cervical canal. The chorion or placenta is normally attached to the bottom or lateral surfaces of the uterus and does not overlap the pharynx in any way. But in some cases they can partially or completely close the internal opening of the cervical canal - it is in this situation that a disorder called "Chorion presentation"
The closure of the cervical canal by the chorion does not have to be complete, therefore there are several types of presentation that characterize the complexity of this condition:
Partial chorion presentation. In such a situation, the developing placenta covers at least two-thirds of the lumen of the cervical canal.
Regional chorionic presentation . This is a variation and, one might say, an easier version of partial presentation, since only one third of the lumen of the pharynx is covered.
Central chorion presentation. In this case, the lumen of the pharynx of the cervical canal is completely closed by the future placenta, which significantly complicates the course of pregnancy and poses a threat to both the unborn child and the life of the mother.
Low location of the chorion . The forming placenta can be located next to the opening of the cervix, but does not block it. If it is attached near the edge of the pharynx closer than three centimeters, then it is said to be low. This is not dangerous, but poses a potential threat to pregnancy.
Chorionic presentation at week 12 can be in any of these forms.
As pregnancy progresses, the growing uterus can pull back the placenta, so central presentation can turn into partial and marginal, and then disappear completely. According to obstetricians, more than 90% of cases of one or another chorionic presentation completely disappear over time, so if you were diagnosed with it in the first weeks of pregnancy, this is not a reason to panic. But you will have to monitor your condition and not neglect examinations by a specialist.
Why exactly the developing placenta is attached in such dangerous proximity to the pharynx of the cervical canal is completely unknown. However, several main factors have been noted that contribute to a greater likelihood of developing this pregnancy complication. Especially often, various variants of chorionic presentation develop in women who have had in the past or currently have the following diseases and conditions:
Inflammatory lesions of the uterus, abortions, especially using the curettage method, surgical interventions for fibroids or cesarean section. All these factors are united by one consequence - after this, scars and adhesions can be left on the inner surface of the uterus, which make it difficult for the chorion to attach to the “right” place.
Diseases of the liver, kidneys or heart. It would seem, how can these conditions affect the position of the fetus and its placenta in the uterus? But with pathologies of these organs, blood stagnation may occur in the pelvic area, which contributes to lower attachment of the chorion.
Multiple births in the past. If you are pregnant not for the first time, then your chances of improper attachment of the chorion significantly increase. Most physiologists see the reasons for this phenomenon in the fact that after each pregnancy, in the area of the uterus where the placenta was attached, the structure of the endometrium changes. Therefore, at the next conception, the chorion can no longer attach there. Over time, such places on the inner surface of the uterus become less and less, which leads to the attachment of the placenta in the danger zone.
Uterine deformities, acquired (for example, after surgical interventions) or congenital in nature, can also lead to chorion presentation.
Most pregnant women are frightened by such a conclusion from the first ultrasound examination. Although in fact, chorionic presentation during pregnancy of 10-13 weeks is observed in approximately 5% of cases, that is, in every twentieth woman. In later stages, this condition becomes increasingly rare, observed before childbirth in no more than 0.5% of women in labor. The main reason for this is that the growing uterus is able to “pull” the chorion attachment point from the cervical canal to a safer area. Therefore, according to pediatricians, chorion presentation during the first trimester can be regarded as a feature of the course of pregnancy, but not a complication.
Difficulties begin if the presentation continues to persist after the third month of pregnancy. Being dangerously close to the pharynx of the cervical canal, the placenta can be easily injured, which leads to bleeding of varying degrees. With marginal or partial presentation, the first spotting occurs closer to the sixth month. They are practically painless, and blood may be released in thin streaks in the discharge, or give the impression of menstruation. Central presentation can manifest itself with such symptoms as early as the second or third month. In fact, this is the main consequence and danger of chorion presentation, which entails a number of disruptions to the course of pregnancy and the health of the mother and her unborn child:
The constant loss of small amounts of blood leads to anemia in a pregnant woman. You may experience weakness, dizziness, and your skin becomes pale. In case of severe bleeding, blood pressure may decrease, vision may become dark, and you may even lose consciousness.
Disruption of connections between the uterus and placenta also leads to malnutrition of the unborn baby. Its development slows down, and against the background of reduced oxygen delivery (due to a damaged placenta and anemia in the mother), intrauterine fetal hypoxia occurs.
If the mother’s blood loss reaches significant levels, this can lead to miscarriage, intrauterine fetal death and a number of other terrible consequences.
In addition to the problems described, presentation is often complicated by incorrect positioning of the fetus, which leads to difficulties during the birth process. Therefore, if such a condition is diagnosed in you in the sixth month or later, then you need to mentally prepare yourself for the fact that you may have to have a caesarean section rather than give birth on your own.
Unfortunately, at the moment, doctors do not yet know how to correct such a condition as chorionic presentation, so all treatment comes down to preventing complications and eliminating their consequences. As a rule, if there is a central presentation in the fourth month, they prefer to place the girl in the position in a hospital for preservation. The same is done with partial forms of presentation, if they are complicated by bleeding, hypertonicity of the uterus and other factors that may threaten termination of pregnancy. In a hospital setting you will be provided with the following treatment:
To begin with, strict bed rest and limitation of physical activity, which is one of the most important factors in the prevention of bleeding during placenta previa. In addition, you will need to avoid and emotional stress, since this can also lead to negative consequences.
Regular examination by a doctor and diagnostic ultrasound examinations. Being under 24-hour medical supervision, you greatly reduce the risk of sudden complications, since they will be identified and corrected as quickly as possible. short term. Most deplorable and even tragic situations with chorion presentation are caused by delayed medical intervention.
Maintenance treatment, which includes all the vitamins necessary for the pregnant body.
Proper and regular nutrition, which normalizes the functioning of the gastrointestinal tract. If you have diarrhea or constipation, you may strain your abdominal muscles, which increases pressure in the pelvis and can trigger bleeding.
If you develop anemia due to bleeding, it can be treated in a hospital setting by taking iron supplements, including those given by injection.
Treatment is also prescribed to eliminate other factors that threaten the course of pregnancy - for example, antispasmodics for uterine hypertonicity.
In case of partial chorionic presentation, which does not manifest itself with severe symptoms, you do not have to go to the preservation, but you need to take certain precautions to prevent possible complications. These primarily include:
Exercise stress. Leisurely walks and walking around the house is the maximum for a girl in such a situation. Lifting heavy objects, walking up stairs, and running are strictly contraindicated.
It is necessary to completely avoid sexual contact. During pregnancy, in principle, sexual intercourse is not prohibited at almost any stage, but during presentation it can cause severe bleeding.
Mental stress or stress affects the pregnant body no better than lifting weights. Therefore, they also need to be excluded, and even with sedentary and predominantly mental work, it will be time for you to go on maternity leave.
Also, as with preservation, it is necessary to eat properly so as not to cause changes in stool and at the same time provide the body with all the necessary nutrients. You also need to agree with your doctor on the choice of a vitamin complex, which will be very useful in such a situation.
And most importantly, if you have been diagnosed with chorion previa and at some point you notice the release of even a small amount of blood in the absence of pain, weakness and other symptoms, then you need to urgently consult a doctor. And if the bleeding is accompanied by pain in the lower back and lower abdomen, palpitations, weakness or fainting, then you need to call “ Ambulance"as soon as possible, as you risk losing your child.

Dream interpretation is an ancient art that allows you to at least assess the psychological status of a person, because...

As soon as the first mirrors were born, people immediately endowed them with all sorts of mystical abilities....

Photo: Anatoly ZHDANOV Understanding the program “The East is a delicate matter” on Radio “Komsomolskaya Pravda” [audio] Juma:...

Interpretation of the dream in the dream book: A man sees how he is being released from prison - the criminal sees great difficulties in life...

Making a new friend in a dream foreshadows the birth of a child. Seeing friends who have been absent for a long time - for the upcoming...

In the context of the implementation of the Federal State Educational Standard, it is of great importance. Over the course of decades, educational institutions have developed a system of work...

The manual discusses programs of domestic and foreign authors that are used in the work...

How often do we see this monster with goat horns when we lay out Tarot cards. "Devil" is the personification of hell...

Navigation: Description and history of the map: To the side of the road there is a large oak tree, in its foliage they find both shelter and food...
Dear forum visitors, I am opening this topic for fans of Patrick Walesa's "Deviant Tarot" deck...
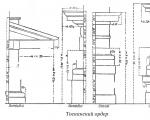
Tuscan order. Tuscan order, one of the five Roman architectural orders. The name is associated with...

LIBRETTO. If you love music (which you undoubtedly do, since you needed this book), then you'll probably...

Religion: paganism Birth: 942 (0942) Death: March on the Dnieper Family: Rurikovich Father:...

Masaccio (actually Tommaso di Giovanni di Simone Cassai (Guidi), Tommaso di ser Giovanni di Guidi; December 21...

As soon as the first mirrors were born, people immediately endowed them with all sorts of mystical abilities....

Photo: Anatoly ZHDANOV We understand the program “The East is a delicate matter” on Radio “Komsomolskaya Pravda” [audio]...